Atendimento especializado em intervenções coronárias complexas
Atención especializada para intervenciones coronarias complejas
What Is Coronary Artery Disease?
Coronary artery disease (CAD) happens when plaque builds up inside the arteries that supply blood to your heart. Think of it like a clogged pipe — the buildup narrows the opening, making it harder for blood to flow through.
When your heart doesn't get enough blood, you might feel chest pain (called angina), shortness of breath, or unusual fatigue. These are signs that your heart is working too hard and not getting enough oxygen.
Healthy Artery vs. Plaque Buildup
The good news: there are treatments that can help restore blood flow to your heart and relieve your symptoms.
O que é Doença Arterial Coronariana?
A doença arterial coronariana (DAC) ocorre quando a placa se acumula dentro das artérias que fornecem sangue para o seu coração. Pense nisso como um cano entupido — o acúmulo estreita a abertura, dificultando o fluxo de sangue.
Quando seu coração não recebe sangue suficiente, você pode sentir dor no peito (chamada angina), falta de ar ou fadiga incomum. Estes são sinais de que seu coração está trabalhando muito e não está recebendo oxigênio suficiente.
Artéria Saudável vs. Acúmulo de Placa
A boa notícia é que existem tratamentos que podem ajudar a restaurar o fluxo sanguíneo para seu coração e aliviar seus sintomas.
¿Qué es la Enfermedad Arterial Coronaria?
La enfermedad arterial coronaria (EAC) ocurre cuando la placa se acumula dentro de las arterias que suministran sangre a su corazón. Piense en ello como una tubería obstruida: la acumulación estrecha la abertura, lo que dificulta el flujo de sangre.
Cuando su corazón no recibe suficiente sangre, puede sentir dolor en el pecho (llamado angina), falta de aire o fatiga inusual. Estos son signos de que su corazón está trabajando demasiado y no está recibiendo suficiente oxígeno.
Arteria Sana vs. Acumulación de Placa
La buena noticia: hay tratamientos que pueden ayudar a restaurar el flujo sanguíneo a su corazón y aliviar sus síntomas.
What Is a Chronic Total Occlusion (CTO)?
A CTO is an artery that is 100% blocked for at least 3 months. "Chronic" means it's been there a long time, and "total occlusion" means completely blocked — no blood flows through it at all.
When this happens, your body is smart: it creates tiny detour blood vessels (called collaterals) around the blockage. But these detours aren't enough to give your heart all the blood it needs.
Many patients are told "nothing can be done" about a CTO. But that's not true anymore. Advanced techniques and specialized training now make it possible to open these blocked arteries safely.
Chronic Total Occlusion (100% Blocked)
O que é uma Oclusão Total Crônica (CTO)?
Uma CTO é uma artéria que está 100% bloqueada há pelo menos 3 meses. "Crônica" significa que está lá há muito tempo, e "oclusão total" significa completamente bloqueada — nenhum sangue flui através dela.
Quando isso acontece, seu corpo se adapta: cria pequenos vasos sanguíneos de desvio (chamados colaterais) ao redor do bloqueio. Mas esses desvios não são suficientes para suprir toda a demanda do seu coração.
Muitos pacientes ouvem que "não há nada a fazer" sobre uma CTO. Isso não é mais verdade. Técnicas avançadas e treinamento especializado agora tornam possível abrir essas artérias bloqueadas com segurança.
Oclusão Total Crônica (100% Bloqueada)
¿Qué es una Oclusión Total Crónica (CTO)?
Una CTO es una arteria que está 100% bloqueada durante al menos 3 meses. "Crónica" significa que ha estado allí durante mucho tiempo, y "oclusión total" significa completamente bloqueada: no fluye sangre a través de ella.
Cuando esto sucede, su cuerpo es inteligente: crea pequeños vasos sanguíneos de derivación (llamados colaterales) alrededor del bloqueo. Pero estas derivaciones no son suficientes para darle a su corazón toda la sangre que necesita.
Muchos pacientes son informados de que "no se puede hacer nada" sobre una CTO. Pero eso ya no es verdad. Las técnicas avanzadas y el entrenamiento especializado ahora hacen posible abrir estas arterias bloqueadas de forma segura.
Oclusión Total Crónica (100% Bloqueada)
How Is Coronary Disease Diagnosed?
Diagnosing coronary artery disease starts with your doctor listening to your symptoms and reviewing your medical history. Common symptoms include chest pain or pressure (angina), shortness of breath, and unusual fatigue, especially with physical activity.
Your doctor may order several tests to evaluate your heart:
Non-Invasive Tests
Electrocardiogram (ECG): A quick test that records your heart's electrical activity. It can show if your heart has been damaged by reduced blood flow.
Echocardiogram: An ultrasound of your heart that shows how well it pumps and whether any areas of the heart muscle are weak (which could mean poor blood supply).
CT Coronary Angiography (CTA): A specialized scan that creates detailed 3D images of your heart's arteries. Beyond simply detecting blockages, CT is particularly valuable for planning CTO procedures: it shows the exact length and shape of the blockage, the amount of calcium present, and helps your doctor choose the best approach and equipment before the procedure even begins.
Stress Testing & Heart Muscle Viability
Before opening a completely blocked artery, your doctor needs to answer two important questions: (1) Is the blockage actually causing reduced blood flow to your heart? and (2) Is the heart muscle in that area still alive and capable of recovering?
Not every blocked artery causes symptoms or needs treatment. Some blockages develop slowly and the heart builds alternative blood supply routes (collaterals). Stress tests help determine whether treatment will truly benefit you.
Cardiac MRI (CMR): The most comprehensive test for CTO patients. It evaluates heart function, blood flow under stress, and most importantly, whether the heart muscle is still viable (alive) or has become scar tissue. This is done using a special contrast agent (gadolinium). If the scar involves less than 50% of the wall thickness, recovery after opening the artery is expected.
PET Scan: A nuclear imaging test that measures both blood flow and metabolic activity of the heart muscle. When an area shows reduced blood flow but preserved metabolic activity (called a "mismatch"), it means the muscle is hibernating and will likely recover after revascularization. PET provides the highest accuracy for viability assessment.
Nuclear Stress Test (SPECT): The most widely available stress imaging test. While less precise than CMR or PET, it effectively detects reduced blood flow and provides a good initial assessment.
Coronary Angiography (Cardiac Catheterization)
If non-invasive tests confirm significant disease, your doctor may recommend a coronary angiogram. A thin, flexible tube (catheter) is inserted through a small puncture in your wrist or groin and guided to your heart. Contrast dye is injected so the arteries can be seen on X-ray. This is the gold standard for identifying the exact location and severity of blockages, and it is often the moment when a CTO is first identified.
Como a Doença Coronariana é Diagnosticada?
O diagnóstico da doença arterial coronariana começa com o médico avaliando seus sintomas e revisando seu histórico clínico. Sintomas comuns incluem dor ou pressão no peito (angina), falta de ar e fadiga incomum, especialmente durante atividade física.
Seu médico pode solicitar diversos exames para avaliar seu coração:
Exames Não Invasivos
Eletrocardiograma (ECG): Um teste rápido que registra a atividade elétrica do seu coração. Pode identificar sinais de sofrimento cardíaco por redução do fluxo sanguíneo.
Ecocardiograma: Uma ultrassonografia do coração que mostra quão bem ele bombeia e se alguma área do músculo cardíaco está fraca (o que pode significar suprimento sanguíneo deficiente).
Angiotomografia Coronariana (AngioTC): Um exame especializado que cria imagens 3D detalhadas das artérias do coração. Além de detectar obstruções, a AngioTC é especialmente valiosa para planejar procedimentos de CTO: mostra o comprimento e formato exato da obstrução, a quantidade de cálcio presente e ajuda o médico a escolher a melhor abordagem e equipamentos antes do procedimento.
Prova Funcional e Viabilidade Miocárdica
Antes de abrir uma artéria completamente bloqueada, seu médico precisa responder duas perguntas importantes: (1) A obstrução está realmente causando redução do fluxo sanguíneo? e (2) O músculo cardíaco nessa região ainda está vivo e capaz de se recuperar?
Nem toda artéria bloqueada causa sintomas ou precisa de tratamento. Algumas obstruções se desenvolvem lentamente e o coração constrói rotas alternativas de suprimento sanguíneo (colaterais). Provas funcionais ajudam a determinar se o tratamento realmente trará benefício.
Ressonância Magnética Cardíaca (RMC): O exame mais completo para pacientes com CTO. Avalia a função cardíaca, o fluxo sanguíneo sob estresse e, mais importante, se o músculo cardíaco ainda é viável (vivo) ou se tornou tecido cicatricial. Isso é feito usando um agente de contraste especial (gadolínio). Se a cicatriz envolver menos de 50% da espessura da parede, a recuperação após abrir a artéria é esperada.
PET Scan: Um exame de imagem nuclear que mede tanto o fluxo sanguíneo quanto a atividade metabólica do músculo cardíaco. Quando uma área mostra fluxo reduzido mas atividade metabólica preservada (chamado "mismatch"), significa que o músculo está hibernando e provavelmente se recuperará após a revascularização. O PET oferece a maior acurácia para avaliação de viabilidade.
Cintilografia Miocárdica (SPECT): O teste de imagem de estresse mais amplamente disponível. Embora menos preciso que RMC ou PET, detecta efetivamente redução do fluxo sanguíneo e fornece uma boa avaliação inicial.
Cateterismo Cardíaco (Coronariografia)
Se os exames não invasivos confirmarem doença significativa, seu médico pode recomendar uma coronariografia. Um tubo fino e flexível (cateter) é inserido através de uma pequena punção no pulso ou virilha e guiado até o coração. Contraste é injetado para que as artérias sejam vistas no raio-X. Este é o padrão-ouro para identificar a localização exata e gravidade das obstruções, e é frequentemente o momento em que uma CTO é identificada pela primeira vez.
¿Cómo se Diagnostica la Enfermedad Coronaria?
El diagnóstico de la enfermedad arterial coronaria comienza con el médico escuchando sus síntomas y revisando su historia clínica. Los síntomas comunes incluyen dolor o presión en el pecho (angina), falta de aire y fatiga inusual, especialmente durante la actividad física.
Su médico puede ordenar varias pruebas para evaluar su corazón:
Pruebas No Invasivas
Electrocardiograma (ECG): Una prueba rápida que registra la actividad eléctrica de su corazón. Puede mostrar si el corazón ha sido dañado por la reducción del flujo sanguíneo.
Ecocardiograma: Una ecografía del corazón que muestra qué tan bien bombea y si alguna área del músculo cardíaco está débil (lo que podría significar suministro sanguíneo deficiente).
Angiotomografía Coronaria (AngioTC): Un examen especializado que crea imágenes 3D detalladas de las arterias del corazón. Además de detectar obstrucciones, la AngioTC es especialmente valiosa para planificar procedimientos de CTO: muestra la longitud y forma exacta de la obstrucción, la cantidad de calcio presente y ayuda al médico a elegir el mejor enfoque y equipamiento antes del procedimiento.
Prueba Funcional y Viabilidad Miocárdica
Antes de abrir una arteria completamente bloqueada, su médico necesita responder dos preguntas importantes: (1) ¿La obstrucción está realmente causando reducción del flujo sanguíneo? y (2) ¿El músculo cardíaco en esa zona todavía está vivo y es capaz de recuperarse?
No toda arteria bloqueada causa síntomas o necesita tratamiento. Algunas obstrucciones se desarrollan lentamente y el corazón construye rutas alternativas de suministro sanguíneo (colaterales). Las pruebas funcionales ayudan a determinar si el tratamiento realmente le beneficiará.
Resonancia Magnética Cardíaca (RMC): El examen más completo para pacientes con CTO. Evalúa la función cardíaca, el flujo sanguíneo bajo estrés y, lo más importante, si el músculo cardíaco todavía es viable (vivo) o se ha convertido en tejido cicatricial. Esto se realiza con un agente de contraste especial (gadolinio). Si la cicatriz compromete menos del 50% del espesor de la pared, se espera recuperación después de abrir la arteria.
PET Scan: Un examen de imagen nuclear que mide tanto el flujo sanguíneo como la actividad metabólica del músculo cardíaco. Cuando un área muestra flujo reducido pero actividad metabólica preservada (llamado "mismatch"), significa que el músculo está hibernando y probablemente se recuperará después de la revascularización. El PET ofrece la mayor precisión para evaluación de viabilidad.
Gammagrafía Miocárdica (SPECT): La prueba de imagen de estrés más ampliamente disponible. Aunque menos precisa que RMC o PET, detecta eficazmente la reducción del flujo sanguíneo y proporciona una buena evaluación inicial.
Cateterismo Cardíaco (Coronariografía)
Si las pruebas no invasivas confirman enfermedad significativa, su médico puede recomendar una coronariografía. Un tubo fino y flexible (catéter) se inserta a través de una pequeña punción en la muñeca o ingle y se guía hasta el corazón. Se inyecta contraste para ver las arterias en rayos X. Este es el estándar de oro para identificar la ubicación exacta y gravedad de las obstrucciones, y es frecuentemente el momento en que una CTO se identifica por primera vez.
How CTO PCI Works
CTO PCI is a specialized procedure to reopen a completely blocked artery. Here's the step-by-step process:
No open surgery needed. The procedure is done through a small puncture in your wrist (or groin). You'll usually stay in the hospital for 1-2 nights. Recovery is quick. Most patients go home the next day and resume normal activities within a week.
Como Funciona a ICP para CTO
A ICP para CTO é um procedimento especializado para reabrir uma artéria completamente bloqueada. Veja o processo passo a passo:
Fio guia → Dilatação por balão → Implante de stent → Fluxo sanguíneo restaurado
Assista: Microcateter cruzando uma lesão CTO
Sem necessidade de cirurgia aberta. O procedimento é feito através de uma pequena punção em seu pulso (ou virilha). Em geral, a internação é de 1 a 2 noites. A recuperação é rápida: a maioria dos pacientes recebe alta no dia seguinte e retoma as atividades habituais em cerca de uma semana.
Cómo Funciona el ICP para CTO
El ICP para CTO es un procedimiento especializado para reabriruna arteria completamente bloqueada. Aquí está el proceso paso a paso:
Alambre guía → Dilatación con globo → Implante de stent → Flujo sanguíneo restaurado
Mira: Microcatéter cruzando una lesión CTO
Sin cirugía abierta necesaria. El procedimiento se realiza a través de una pequeña punción en su muñeca (o ingle). Generalmente permanecerá en el hospital durante 1-2 noches. La recuperación es rápida. La mayoría de los pacientes salen al día siguiente y reanudan las actividades normales en una semana.
The CTO PCI Procedure: What to Expect
Risks vs. Benefits
Like any medical procedure, CTO PCI has both risks and benefits. The main benefits include relief from chest pain and shortness of breath, improved exercise capacity, reduced need for multiple medications, and in many cases, an alternative to open-heart bypass surgery.
The risks are low in experienced hands but include bleeding at the access site, allergic reaction to contrast dye, kidney stress from contrast, damage to the artery, and in rare cases (less than 1%), heart attack or need for emergency surgery. Your doctor will discuss your individual risk profile before the procedure.
Dual and Triple Arterial Access
Unlike a standard angioplasty that uses one catheter, CTO PCI often requires two or even three access points. This means your doctor may place catheters in both wrists, or one in the wrist and one in the groin. The reason is that the blocked artery needs to be seen from both sides simultaneously: one catheter injects dye into the artery before the blockage, while another shows the artery beyond the blockage through collateral vessels (the natural detours your body created).
This "dual injection" technique is essential for the operator to navigate safely through the blockage.
Retrograde Approach
Sometimes the blockage is too hard or too long to cross from the front (antegrade approach). In these cases, your doctor may use a "retrograde" strategy: instead of pushing through the blockage from the beginning, a tiny wire and microcatheter are threaded through the collateral vessels (natural detour pathways) to reach the blockage from the other side. This advanced technique significantly increases the chances of success in the most challenging cases.
O Procedimento de ICP para CTO: O que Esperar
Riscos vs. Benefícios
Como qualquer procedimento médico, a ICP para CTO tem riscos e benefícios. Os principais benefícios incluem alívio da dor no peito e da falta de ar, melhora na capacidade de exercício, redução da necessidade de múltiplos medicamentos e, em muitos casos, uma alternativa à cirurgia de revascularização miocárdica (ponte de safena).
Os riscos são baixos em mãos experientes, mas incluem sangramento no local de acesso, reação alérgica ao contraste, estresse renal pelo contraste, dano à artéria e, em casos raros (menos de 1%), infarto ou necessidade de cirurgia de emergência. Seu médico discutirá os riscos e benefícios específicos para o seu caso antes do procedimento.
Acesso Arterial Duplo e Triplo
Diferente de uma angioplastia convencional que utiliza um único cateter, a ICP para CTO frequentemente requer dois ou até três pontos de acesso. Isso significa que o médico pode inserir cateteres nos dois pulsos, ou um no pulso e outro na virilha. A razão é que a artéria bloqueada precisa ser vista dos dois lados simultaneamente: um cateter injeta contraste na artéria antes do bloqueio, enquanto outro mostra a artéria além do bloqueio através dos vasos colaterais (os desvios naturais que o corpo criou).
Essa técnica de "dupla injeção" é essencial para o operador navegar com segurança através do bloqueio.
Abordagem Retrógrada
Em alguns casos, o bloqueio é muito resistente ou extenso para ser cruzado pela frente (abordagem anterógrada). Nestes casos, o médico pode usar uma estratégia "retrógrada": em vez de empurrar através do bloqueio pelo início, um fio-guia e microcateter são avançados através dos vasos colaterais (caminhos de desvio naturais) para acessar o bloqueio pelo lado oposto. Esta técnica avançada aumenta significativamente as chances de sucesso nos casos mais desafiadores.
El Procedimiento de ICP para CTO: Qué Esperar
Riesgos vs. Beneficios
Como cualquier procedimiento médico, el ICP para CTO tiene riesgos y beneficios. Los principales beneficios incluyen alivio del dolor torácico y la falta de aire, mejora en la capacidad de ejercicio, reducción de la necesidad de múltiples medicamentos y, en muchos casos, una alternativa a la cirugía de bypass.
Los riesgos son bajos en manos experimentadas, pero incluyen sangrado en el sitio de acceso, reacción alérgica al contraste, estrés renal por contraste, daño a la arteria y, en casos raros (menos del 1%), infarto o necesidad de cirugía de emergencia. Su médico discutirá su perfil de riesgo individual antes del procedimiento.
Acceso Arterial Doble y Triple
A diferencia de una angioplastia estándar que usa un catéter, el ICP para CTO frecuentemente requiere dos o hasta tres puntos de acceso. Esto significa que el médico puede colocar catéteres en ambas muñecas, o uno en la muñeca y otro en la ingle. La razón es que la arteria bloqueada necesita verse desde ambos lados simultáneamente: un catéter inyecta contraste en la arteria antes del bloqueo, mientras otro muestra la arteria más allá del bloqueo a través de los vasos colaterales (los desvíos naturales que el cuerpo creó).
Esta técnica de "doble inyección" es esencial para que el operador navegue con seguridad a través del bloqueo.
Abordaje Retrógrado
A veces el bloqueo es demasiado duro o demasiado largo para cruzar por el frente (abordaje anterógrado). En estos casos, el médico puede usar una estrategia "retrógrada": en vez de empujar a través del bloqueo desde el inicio, un alambre y microcatéter diminutos se guían a través de los vasos colaterales (vías de desvío naturales) para alcanzar el bloqueo desde el otro lado. Esta técnica avanzada aumenta significativamente las posibilidades de éxito en los casos más desafiantes.
Complex & High-Risk PCI
Some patients have disease in multiple arteries, heavily calcified arteries (hardened and stiff), or blockages in the left main artery (which is critical). These are complex cases that require advanced skills and special tools.
These procedures may use special techniques like atherectomy (a tool that shaves away calcified plaque) or imaging technology (IVUS or OCT, which are like "ultrasound" cameras that let us see exactly what we're treating). These advanced interventions can be an alternative to bypass surgery in many cases.
Coronary Intervention with Mechanical Circulatory Support (Impella)
ICP Complexa e de Alto Risco
Alguns pacientes têm doença em múltiplas artérias, artérias fortemente calcificadas (endurecidas e rígidas) ou bloqueios na artéria principal esquerda (que é crítica). Estes são casos complexos que requerem habilidades avançadas e ferramentas especiais.
Esses procedimentos podem usar técnicas especiais como aterectomia (uma ferramenta que raspa a placa calcificada) ou tecnologia de imagem (IVUS ou OCT, que são como câmeras de "ultrassom" que nos permitem ver exatamente o que estamos tratando). Estas intervenções avançadas podem ser uma alternativa à cirurgia de bypass em muitos casos.
Intervenção Coronária com Suporte Circulatório (Impella)
ICP Complejo y de Alto Riesgo
Algunos pacientes tienen enfermedad en múltiples arterias, arterias altamente calcificadas (endurecidas y rígidas) o bloqueos en la arteria principal izquierda (que es crítica). Estos son casos complejos que requieren habilidades avanzadas y herramientas especiales.
Estos procedimientos pueden usar técnicas especiales como aterectomía (una herramienta que raspa la placa calcificada) o tecnología de imágenes (IVUS u OCT, que son como cámaras de "ultrasonido" que nos permiten ver exactamente lo que estamos tratando). Estas intervenciones avanzadas pueden ser una alternativa al bypass en muchos casos.
Intervención Coronaria con Soporte Circulatorio (Impella)
Recovery After CTO PCI
Most patients stay in the hospital for one night after the procedure. If dual access was used (wrist and groin), you may need to lie flat for a few hours until the groin access site seals.
First Week
You can resume light daily activities (walking, light housework) within 1 to 2 days. Avoid heavy lifting (more than 10 pounds) and intense exercise for about one week. Keep the access sites clean and dry. Some bruising at the wrist or groin is normal.
Medications
You will be prescribed dual antiplatelet therapy (typically aspirin plus a second blood thinner such as clopidogrel, prasugrel, or ticagrelor). It is critical that you take these medications exactly as prescribed. Stopping them too early can cause the new stent to clot, which is a medical emergency. Most patients take dual therapy for at least 12 months.
Follow-Up
You will typically see your cardiologist 2 to 4 weeks after the procedure, then again at 3, 6, and 12 months. A stress test may be performed at 6 to 12 months to confirm that blood flow remains good.
Long-Term Outlook
Many patients notice improvement in their symptoms within days. Studies show that successful CTO PCI improves quality of life, reduces angina, and may improve long-term survival. The key to lasting results is taking your medications, managing risk factors (blood pressure, cholesterol, diabetes, smoking), and staying physically active.
Recuperação Após ICP para CTO
A maioria dos pacientes fica no hospital por uma noite após o procedimento. Se foi utilizado acesso duplo (pulso e virilha), pode ser necessário permanecer deitado por algumas horas até que o local de acesso na virilha cicatrize.
Primeira Semana
Você pode retomar atividades diárias leves (caminhada, tarefas domésticas leves) em 1 a 2 dias. Evite carregar peso acima de 5 kg e exercícios intensos por cerca de uma semana. Mantenha os locais de acesso limpos e secos. Pequenos hematomas no local de acesso são normais.
Medicamentos
Você receberá prescrição de dupla antiagregação plaquetária (tipicamente aspirina mais um segundo antiagregante plaquetário como clopidogrel, prasugrel ou ticagrelor). É fundamental seguir a prescrição rigorosamente. A interrupção precoce pode causar trombose do stent, uma complicação grave. Em geral, a terapia dupla é mantida por pelo menos 12 meses.
Acompanhamento
Você normalmente consultará seu cardiologista 2 a 4 semanas após o procedimento, depois novamente em 3, 6 e 12 meses. Uma prova funcional pode ser realizada em 6 a 12 meses para confirmar que o fluxo sanguíneo permanece bom.
Perspectiva a Longo Prazo
Muitos pacientes notam melhora nos sintomas em poucos dias. Estudos mostram que a ICP para CTO bem-sucedida melhora a qualidade de vida, reduz a angina e pode melhorar a sobrevida a longo prazo. A chave para resultados duradouros é tomar seus medicamentos, controlar fatores de risco (pressão arterial, colesterol, diabetes, tabagismo) e manter-se fisicamente ativo.
Recuperación Después del ICP para CTO
La mayoría de los pacientes permanecen en el hospital una noche después del procedimiento. Si se usó acceso doble (muñeca e ingle), puede necesitar permanecer acostado por algunas horas hasta que el sitio de acceso inguinal cicatrice.
Primera Semana
Puede retomar actividades diarias ligeras (caminar, tareas domésticas ligeras) en 1 a 2 días. Evite levantar peso (más de 5 kg) y ejercicio intenso por aproximadamente una semana. Mantenga los sitios de acceso limpios y secos. Algo de moretón en la muñeca o ingle es normal.
Medicamentos
Se le prescribirá doble antiagregación plaquetaria (típicamente aspirina más un segundo anticoagulante como clopidogrel, prasugrel o ticagrelor). Es fundamental que tome estos medicamentos exactamente como se le indique. Dejar de tomarlos demasiado pronto puede causar trombosis del stent, lo cual es una emergencia médica. La mayoría de los pacientes toman la terapia doble por al menos 12 meses.
Seguimiento
Normalmente verá a su cardiólogo 2 a 4 semanas después del procedimiento, luego nuevamente a los 3, 6 y 12 meses. Una prueba de esfuerzo puede realizarse a los 6 a 12 meses para confirmar que el flujo sanguíneo permanece bueno.
Perspectiva a Largo Plazo
Muchos pacientes notan mejoría en sus síntomas en pocos días. Los estudios muestran que el ICP para CTO exitoso mejora la calidad de vida, reduce la angina y puede mejorar la supervivencia a largo plazo. La clave para resultados duraderos es tomar sus medicamentos, controlar factores de riesgo (presión arterial, colesterol, diabetes, tabaquismo) y mantenerse físicamente activo.
How Dr. Martins Filho Can Help
Dr. Evandro Martins Filho is an interventional cardiologist with specialized fellowship training in CTO PCI. He performs over 600 PCI procedures each year and is recognized as a CTO specialist.
Whether you've been told your condition can't be treated, or you want a second opinion, Dr. Martins Filho can help evaluate your options.
To schedule a consultation: Have your doctor refer you, or contact us through the main website with your recent angiography films.
Dr. Evandro Martins Filho é um cardiologista intervencionista com treinamento especializado em ICP para CTO. Ele realiza mais de 600 procedimentos de ICP por ano e é reconhecido como um especialista em CTO.
Se você foi informado de que sua condição não pode ser tratada, ou deseja uma segunda opinião, o Dr. Martins Filho pode ajudá-lo a avaliar suas opções.
Para agendar uma consulta: Peça ao seu médico para encaminhá-lo ou entre em contato pelo site principal com seus exames de coronariografia recentes.
Dr. Evandro Martins Filho es un cardiólogo intervencionista con entrenamiento especializado en ICP para CTO. Realiza más de 600 procedimientos de ICP cada año y es reconocido como especialista en CTO.
Si le han dicho que su condición no puede ser tratada, o desea una segunda opinión, el Dr. Martins Filho puede ayudarle a evaluar sus opciones.
Para programar una consulta: Pida a su médico que lo refiera, o contáctenos a través del sitio web principal con sus angiogramas recientes.
The EURO-CTO trial demonstrated high success rates (>85%) with modern hybrid algorithms in experienced centers, with favorable long-term outcomes including symptom relief and reduced medication burden. The DECISION-CTO trial showed improved symptoms and exercise capacity following successful CTO PCI. Success rates with current techniques exceed 85% in high-volume centers. Lesion complexity assessment using the J-CTO score and PROGRESS-CTO score helps predict success and risk stratification.
Hybrid Algorithm Approach
Antegrade Wire Escalation (AWE): Sequential escalation of wire stiffness and support to cross lesions. Optimized for lesions with moderate complexity and calcification.
Antegrade Dissection Re-entry (ADR): Intentional wire or microcatheter dissection creating a subintimal space proximal to the occlusion, with re-entry distal to it. Effective for calcified, ambiguous, or tortuous lesions.
Retrograde Approach: Via collateral vessels, particularly useful when anterograde approaches fail. Requires collateral assessment and specialized techniques. Modern retrograde techniques have expanded the population of recanalizable CTOs significantly.
Before: Complete Occlusion
After: Flow Restored
ICP para CTO: Indicações, Técnicas e Resultados
Evidências e Resultados
O registro EURO-CTO demonstrou taxas de sucesso superiores a 85% com o algoritmo híbrido em centros especializados, com alívio sustentado de sintomas e redução da carga medicamentosa. O estudo DECISION-CTO demonstrou melhora sintomática e de capacidade funcional após recanalização bem-sucedida. Com as técnicas atuais, as taxas de sucesso excedem 85% em centros de alto volume. Os escores J-CTO e PROGRESS CTO auxiliam na predição de sucesso e estratificação de risco.
Algoritmo Híbrido
Escalada Anterógrada de Fio-guia (AWE): Escalada sequencial de rigidez de fio-guia e suporte para atravessar lesões. Otimizada para lesões de complexidade e calcificação moderadas.
Dissecção Anterógrada e Reentrada (ADR): Dissecção intencional de fio-guia ou microcateter criando espaço subintimal proximal à oclusão, com re-entrada distal a ela. Indicada para lesões calcificadas, com coto ambíguo ou tortuosidade significativa.
Abordagem Retrógrada: Via vasos colaterais, particularmente útil quando as abordagens anterógradas falham. Requer avaliação colateral e técnicas especializadas. As técnicas retrógradas contemporâneas ampliaram significativamente o espectro de CTOs recanalizáveis.
Antes: Oclusão Completa
Depois: Fluxo Restaurado
ICP para CTO: Indicaciones, Técnicas y Resultados
Evidencia y Resultados
El EURO-CTO demostró altas tasas de éxito (>85%) con algoritmos híbridos modernos en centros experimentados, con resultados favorables a largo plazo incluyendo alivio de síntomas y reducción de la carga de medicamentos. El ensayo DECISION-CTO mostró mejora de síntomas y capacidad de ejercicio después de ICP exitosa para CTO. Las tasas de éxito con técnicas actuales superan el 85% en centros de alto volumen. La evaluación de la complejidad de lesiones usando la puntuación J-CTO y la puntuación PROGRESS-CTO ayuda a predecir el éxito y la estratificación del riesgo.
Enfoque del Algoritmo Híbrido
Escalada de Alambre Anterógrado (AWE): Escalada secuencial de rigidez de alambre y soporte para cruzar lesiones. Optimizado para lesiones con complejidad y calcificación moderadas.
Disección Anterógrada y Reentrada (ADR): Disección intencional de alambre o microcatéter creando espacio subintimal proximal a la oclusión, con reentrada distal a ella. Efectivo para lesiones calcificadas, ambiguas o tortuosas.
Enfoque Retrógrado: A través de vasos colaterales, particularmente útil cuando los enfoques anterógrados fracasan. Requiere evaluación colateral y técnicas especializadas. Las técnicas retrógradas modernas han expandido significativamente la población de CTOs recanalizables.
Antes: Oclusión Completa
Después: Flujo Restaurado
Pre-Procedural Evaluation & Functional Testing
Comprehensive CTO PCI planning integrates two complementary assessments that answer fundamentally different questions: (1) Should we attempt CTO PCI? (answered by ischemia/viability testing) and (2) How should we perform CTO PCI? (answered by CT anatomical planning).
Stress Testing & Viability Assessment
Non-invasive stress imaging is the gatekeeper for patient selection, providing three critical pieces of information: presence and extent of inducible ischemia, myocardial viability in the CTO territory, and global LV function/volumes.
Cardiac MRI (CMR): Reference standard for myocardial tissue characterization. The CMR stress protocol includes cine function, stress/rest perfusion (adenosine/regadenoson), LGE viability, and T1/T2 mapping. LGE transmurality is the cornerstone of viability assessment: segments with <50% transmural scar are considered viable with reasonable expectation of functional recovery; segments with >50% transmural LGE are unlikely to improve even after successful recanalization. Native T1 mapping and ECV fraction detect diffuse interstitial fibrosis beyond what LGE can identify. CMR sensitivity for ischemia detection: 89-91%, specificity: 80-85% (CE-MARC analysis, Bisaccia et al. 2025).
PET Myocardial Perfusion & Viability: Highest sensitivity/specificity for viability assessment through simultaneous evaluation of myocardial blood flow (perfusion) and metabolic activity (glucose utilization). The flow-metabolism MISMATCH pattern (reduced flow + preserved FDG uptake) identifies hibernating viable myocardium. Perfusion tracers: Rb-82 (generator-produced, 75s half-life, quantitative MBF in mL/min/g), N-13 Ammonia (cyclotron-produced, gold standard for quantitative MBF), O-15 Water (most accurate for absolute MBF). The 18F-FDG viability protocol requires fasting 6-12h, glucose loading, target blood glucose 100-140 mg/dL before injection, 45-60 min uptake period. Rb-82 kinetic analysis (k2 washout rate, K1/k2 ratio) can differentiate hibernating myocardium from scar without FDG, achieving 86% concordance with FDG-based viability categorization.
SPECT: Most widely available. Rest-redistribution provides limited viability assessment. Sensitivity for ischemia: 76-82%, specificity: 64-72%. Best for initial screening when CMR/PET access is limited.
Evidence: Viability & Ischemia in CTO PCI Decision-Making
The indication for CTO PCI fundamentally presupposes viability and ischemia in the target territory, combined with refractory symptoms despite optimal medical therapy. This triad (viability + ischemia + symptoms) forms the rationale for intervention.
REVIVED-BCIS2 (NEJM, 2023) reported that viability characteristics did not influence the effect of PCI on prognosis or LV function in severe ischemic cardiomyopathy (EF ≤35%). However, this trial has significant limitations when extrapolated to CTO practice: it enrolled patients with extensive multivessel CAD and severe LV dysfunction (not isolated CTOs), the population had advanced remodeling where recovery potential is inherently limited, PCI technique and completeness of revascularization were not standardized, and the trial was not powered to detect differences in subgroups with preserved EF or single-vessel CTO. REVIVED does not negate the role of viability testing in CTO; rather, it reinforces that patient selection must integrate viability status, ischemic burden, symptom severity, and anatomical complexity.
The ISCHEMIA trial (NEJM, 2020) showed no mortality benefit from routine invasive strategy but demonstrated significantly greater symptom improvement with PCI, particularly in patients with more severe angina.
ORBITA-CTO (JACC, 2026; Al-Lamee et al.): This landmark sham-controlled trial randomized 50 patients with single-vessel CTO, confirmed ischemia/viability, stable angina, and J-CTO ≤3 to CTO PCI vs. placebo procedure. At 6-month follow-up, CTO PCI significantly improved angina symptom score (OR 4.4; 95% CrI 1.6-12.7; Pr[Benefit]=0.996), with ~31 additional angina-free days vs. sham. Quality of life and CCS class also improved. Technical success was 96%, with ~30% requiring retrograde approach. No deaths, MI, or withdrawals for worsening angina occurred. Limitations: highly selected population (single-vessel disease, J-CTO ≤3, experienced operators), small sample size (n=50). Nevertheless, ORBITA-CTO provides the first placebo-controlled evidence that CTO PCI produces genuine symptomatic benefit beyond placebo effect in patients with documented ischemia and viability.
CT Coronary Angiography for CTO Planning
CCTA has transformed pre-procedural CTO planning by providing 3D anatomical information unavailable from conventional angiography. Key advantages include: superior calcification quantification (independent of viewing angle), better proximal cap definition (especially in heavily calcified/ambiguous caps), precise occlusion length measurement, 3D vessel course and tortuosity assessment, and evaluation of the CTO segment relationship with adjacent structures.
CT Morphological Assessment: Four critical features evaluated: (1) Proximal cap: tapered caps favor antegrade wire escalation; blunt/ambiguous caps may require subintimal techniques (ADR/knuckle wire) or retrograde approach; CT can detect micro-channels invisible on angiography. (2) Occlusion body: length (< or >20mm), calcification extent (calcium arc, length, density in Hounsfield units), microchannels. (3) Tortuosity: 3D assessment uniquely enabled by CT, as angulated bends may be foreshortened on standard projections. (4) Distal cap/vessel: vessel quality, landing zone size, branch anatomy for ADR re-entry planning.
CTO Scoring Systems: J-CTO (Morino, 2011): blunt cap, calcification, tortuosity >45°, length ≥20mm, prior failed attempt; 0-5 points (0=Easy 88%, ≥3=Very Difficult 10%). CT-RECTOR (Opolski, 2015): CT-specific score with superior calcification assessment and true 3D tortuosity measurement; adds value over angiography-only scores for heavily calcified or ambiguous CTOs. PROGRESS CTO (Christopoulos, 2016): proximal tortuosity, cap ambiguity, CX location, no interventional collaterals; PPV 87%. CASTLE (Alessandrino, 2019): incorporates patient factors (age, prior CABG); 0-6 points, PPV 87%.
Advanced CT Techniques: Dual injection CT (biphasic/sequential contrast protocol) simultaneously opacifies proximal and distal vessels for complete CTO roadmap. 3D reconstruction and virtual planning (Synapse Vincent, Ziostation, Vitrea) enables virtual path tracing, re-entry zone identification, and retrograde planning with septal course visualization. CT-angiography fusion overlay provides real-time CT roadmap during fluoroscopy. Digital twin computational modeling (FFR-CT concept applied to CTO) is emerging at specialized centers.
How CT Changes Procedural Strategy
Approach selection: blunt/ambiguous cap with heavy calcification → favor retrograde or ADR over antegrade wire escalation. Wire selection: microchannel in cap or tapered morphology → start with soft polymer-jacketed wire (Fielder XT-A, Gladius). Equipment preparation: >270° calcium arc → have RotaPro/orbital atherectomy or IVL ready. Re-entry planning: landing zone 15mm proximal to PDA takeoff → set Stingray balloon target. Collateral assessment: septal course and epicardial collateral size → select retrograde channel. Risk assessment: CT-RECTOR ≥3 or J-CTO ≥3 with calcification → plan for prolonged case, discuss staged approach, ensure MCS availability.
Practical Decision Matrix
Viable + Ischemic (LGE <50%, stress defect): Strong indication for CTO PCI. Proceed with CT planning.
Viable + No Ischemia (LGE <50%, no defect): Consider CTO PCI for symptoms. Benefit mainly symptomatic (angina, exercise tolerance).
Non-viable + Ischemic (LGE >50%, stress defect): Relative contraindication. Limited functional recovery expected. PCI if refractory angina or arrhythmia substrate.
Non-viable + No Ischemia (LGE >50%, matched defect): CTO PCI not recommended. Transmural scar, no ischemia. Consider ICD evaluation.
Avaliação Pré-Procedimento e Prova Funcional
O planejamento abrangente da ICP para CTO integra duas avaliações complementares que respondem questões fundamentalmente diferentes: (1) Devemos tentar a ICP da CTO? (respondido pela prova funcional/viabilidade) e (2) Como devemos realizar a ICP da CTO? (respondido pelo planejamento anatômico por TC).
Prova Funcional e Avaliação de Viabilidade
A imagem de estresse não invasiva é determinante para a seleção de pacientes, fornecendo três informações críticas: presença e extensão de isquemia induzível, viabilidade miocárdica no território da CTO e função/volumes globais do VE.
Ressonância Magnética Cardíaca (RMC): Padrão de referência para caracterização tecidual miocárdica. O protocolo de estresse inclui cine função, perfusão estresse/repouso (adenosina/regadenosona), viabilidade por LGE e mapeamento T1/T2. A transmuralidade do LGE é a pedra angular da avaliação de viabilidade: segmentos com <50% de cicatriz transmural são considerados viáveis com expectativa razoável de recuperação funcional; segmentos com >50% de LGE transmural dificilmente melhoram mesmo após recanalização bem-sucedida. Mapeamento nativo de T1 e fração de ECV detectam fibrose intersticial difusa além do que o LGE identifica. Sensibilidade da RMC para detecção de isquemia: 89-91%, especificidade: 80-85% (análise CE-MARC, Bisaccia et al. 2025).
PET Perfusão Miocárdica e Viabilidade: Maior sensibilidade/especificidade para viabilidade através da avaliação simultânea de fluxo sanguíneo miocárdico (perfusão) e atividade metabólica (utilização de glicose). O padrão MISMATCH fluxo-metabolismo (fluxo reduzido + captação de FDG preservada) identifica miocárdio hibernante viável. Traçadores de perfusão: Rb-82 (gerador, meia-vida 75s, MBF quantitativo em mL/min/g), N-13 Amônia (ciclotron, padrão-ouro para MBF quantitativo), O-15 Água (mais preciso para MBF absoluto). Protocolo de viabilidade com 18F-FDG: jejum 6-12h, carga de glicose, glicemia-alvo 100-140 mg/dL antes da injeção, período de captação 45-60 min. Análise cinética do Rb-82 (taxa de washout k2, razão K1/k2) diferencia miocárdio hibernante de cicatriz sem FDG, com 86% de concordância com a categorização de viabilidade por FDG.
SPECT: Mais amplamente disponível. Repouso-redistribuição fornece avaliação limitada de viabilidade. Sensibilidade para isquemia: 76-82%, especificidade: 64-72%. Melhor para rastreamento inicial quando acesso a RMC/PET é limitado.
Evidência: Viabilidade e Isquemia na Decisão de ICP para CTO
A indicação de ICP para CTO pressupõe fundamentalmente viabilidade e isquemia no território-alvo, combinadas com sintomas refratários apesar de terapia médica otimizada. Essa tríade (viabilidade + isquemia + sintomas) forma a base racional para a intervenção.
O REVIVED-BCIS2 (NEJM, 2023) reportou que características de viabilidade não influenciaram o efeito da ICP no prognóstico ou função do VE na cardiomiopatia isquêmica grave (FE ≤35%). Entretanto, este estudo tem limitações significativas quando extrapolado para a prática de CTO: incluiu pacientes com DAC multiarterial extensa e disfunção grave do VE (não CTOs isoladas), a população apresentava remodelamento avançado com potencial de recuperação inerentemente limitado, a técnica de ICP e completude da revascularização não foram padronizadas, e o estudo não tinha poder para detectar diferenças em subgrupos com FE preservada ou CTO de vaso único. O REVIVED não anula o papel da avaliação de viabilidade na CTO; reforça que a seleção de pacientes deve integrar status de viabilidade, carga isquêmica, gravidade dos sintomas e complexidade anatômica.
O estudo ISCHEMIA (NEJM, 2020) não mostrou benefício de mortalidade da estratégia invasiva de rotina, mas demonstrou melhora sintomática significativamente maior com ICP, particularmente em pacientes com angina mais grave.
ORBITA-CTO (JACC, 2026; Al-Lamee et al.): Este estudo sham-controlado randomizou 50 pacientes com CTO de vaso único, isquemia/viabilidade confirmadas, angina estável e J-CTO ≤3 para ICP de CTO vs. procedimento placebo. No seguimento de 6 meses, a ICP de CTO melhorou significativamente o escore de sintomas de angina (OR 4,4; ICr 95% 1,6-12,7; Pr[Benefício]=0,996), com ~31 dias adicionais livres de angina vs. sham. Qualidade de vida e classe CCS também melhoraram. Sucesso técnico foi 96%, com ~30% necessitando abordagem retrógrada. Sem mortes, IAM ou retiradas por piora da angina. Limitações: população altamente selecionada (vaso único, J-CTO ≤3, operadores experientes), amostra pequena (n=50). Ainda assim, o ORBITA-CTO fornece a primeira evidência placebo-controlada de que a ICP de CTO produz benefício sintomático genuíno além do efeito placebo em pacientes com isquemia e viabilidade documentadas.
Angiotomografia Coronariana para Planejamento de CTO
A TCMD transformou o planejamento pré-procedural de CTO fornecendo informação anatômica 3D indisponível pela angiografia convencional. Vantagens: quantificação superior de calcificação, melhor definição do coto proximal (especialmente em caps calcificados/ambíguos), medição precisa do comprimento da oclusão, avaliação 3D do trajeto e tortuosidade do vaso, e avaliação da relação do segmento CTO com estruturas adjacentes.
Avaliação Morfológica por TC: Quatro características críticas: (1) Coto proximal: tapered favorece escalada anterógrada; blunt/ambíguo pode requerer técnicas subintimais (ADR/knuckle wire) ou retrógrada; TC detecta micro-canais invisíveis na angiografia. (2) Corpo da oclusão: comprimento, extensão de calcificação (arco de cálcio, comprimento, densidade em Hounsfield), micro-canais. (3) Tortuosidade: avaliação 3D exclusiva da TC. (4) Cap distal/vaso: qualidade do vaso, tamanho da landing zone, anatomia de ramos para planejamento de reentrada ADR.
Escores de Complexidade: J-CTO (Morino, 2011): cap abrupto, calcificação, tortuosidade >45°, comprimento ≥20mm, tentativa prévia; 0-5 pontos (0=Fácil 88%, ≥3=Muito Difícil 10%). CT-RECTOR (Opolski, 2015): escore específico de TC com melhor avaliação de calcificação e tortuosidade 3D. PROGRESS CTO (Christopoulos, 2016): tortuosidade proximal, ambiguidade do cap, localização CX, sem colaterais intervencionistas; VPP 87%. CASTLE (Alessandrino, 2019): incorpora fatores do paciente (idade, CABG prévio); 0-6 pontos, VPP 87%.
Técnicas Avançadas de TC: TC com dupla injeção (protocolo de contraste bifásico/sequencial) opacifica simultaneamente vasos proximal e distal para mapeamento anatômico completo. Reconstrução 3D e planejamento virtual (Synapse Vincent, Ziostation, Vitrea) permite traçado de trajeto virtual, identificação de zona de reentrada e planejamento retrógrado com visualização do trajeto septal. Fusão TC-angiografia fornece mapeamento anatômico em tempo real durante fluoroscopia.
Como a TC Muda a Estratégia Procedural
Seleção de abordagem: cap blunt/ambíguo com calcificação pesada → favorecer retrógrada ou ADR. Seleção de fio: micro-canal no cap ou morfologia tapered → iniciar com fio polymer-jacketed (Fielder XT-A, Gladius). Preparação de equipamento: arco de cálcio >270° → RotaPro/aterectomia orbital ou IVL prontos. Planejamento de reentrada: landing zone 15mm proximal ao takeoff da PDA → alvo para Stingray. Avaliação de colaterais: trajeto septal e tamanho de colateral epicárdica → selecionar canal retrógrado. Avaliação de risco: CT-RECTOR ≥3 ou J-CTO ≥3 com calcificação → planejar caso prolongado, discutir abordagem em etapas, garantir disponibilidade de SCM.
Matriz de Decisão Prática
Viável + Isquêmico (LGE <50%, defeito ao estresse): Indicação forte para ICP de CTO. Prosseguir com planejamento por TC.
Viável + Sem Isquemia (LGE <50%, sem defeito): Considerar ICP de CTO para sintomas. Benefício principalmente sintomático.
Não-viável + Isquêmico (LGE >50%, defeito ao estresse): Contraindicação relativa. Recuperação funcional limitada. ICP se angina refratária ou substrato arrítmico.
Não-viável + Sem Isquemia (LGE >50%, defeito matched): ICP de CTO não recomendada. Cicatriz transmural, sem isquemia. Considerar avaliação de CDI.
Evaluación Pre-Procedimiento y Prueba Funcional
La planificación integral del ICP para CTO integra dos evaluaciones complementarias que responden preguntas fundamentalmente diferentes: (1) ¿Debemos intentar el ICP de la CTO? (respondido por la prueba funcional/viabilidad) y (2) ¿Cómo debemos realizar el ICP de la CTO? (respondido por la planificación anatómica por TC).
Prueba Funcional y Evaluación de Viabilidad
La imagen de estrés no invasiva es el gatekeeper para selección de pacientes, proporcionando tres datos críticos: presencia y extensión de isquemia inducible, viabilidad miocárdica en el territorio de la CTO y función/volúmenes globales del VI.
Resonancia Magnética Cardíaca (RMC): Estándar de referencia para caracterización tisular miocárdica. El protocolo de estrés incluye cine función, perfusión estrés/reposo (adenosina/regadenosona), viabilidad por LGE y mapeo T1/T2. La transmuralidad del LGE es la piedra angular de la evaluación de viabilidad: segmentos con <50% de cicatriz transmural son considerados viables con expectativa razonable de recuperación funcional; segmentos con >50% de LGE transmural difícilmente mejoran incluso tras recanalización exitosa. Sensibilidad de la RMC para detección de isquemia: 89-91%, especificidad: 80-85% (análisis CE-MARC, Bisaccia et al. 2025).
PET Perfusión Miocárdica y Viabilidad: Mayor sensibilidad/especificidad para viabilidad mediante evaluación simultánea de flujo sanguíneo miocárdico y actividad metabólica. El patrón MISMATCH flujo-metabolismo (flujo reducido + captación de FDG preservada) identifica miocardio hibernante viable. Trazadores: Rb-82 (generador, vida media 75s, MBF cuantitativo), N-13 Amoníaco (ciclotrón, estándar de oro para MBF), O-15 Agua (más preciso para MBF absoluto). Análisis cinético del Rb-82 (tasa de washout k2, razón K1/k2) diferencia miocardio hibernante de cicatriz sin FDG, con 86% de concordancia.
SPECT: Más ampliamente disponible. Sensibilidad para isquemia: 76-82%, especificidad: 64-72%. Mejor para screening inicial cuando el acceso a RMC/PET es limitado.
Evidencia: Viabilidad e Isquemia en la Decisión de ICP para CTO
La indicación del ICP para CTO presupone fundamentalmente viabilidad e isquemia en el territorio objetivo, combinadas con síntomas refractarios a pesar de terapia médica optimizada. Esta tríada (viabilidad + isquemia + síntomas) forma la base racional de la intervención.
El REVIVED-BCIS2 (NEJM, 2023) reportó que las características de viabilidad no influyeron en el efecto del ICP sobre el pronóstico o la función del VI en cardiomiopatía isquémica severa (FE ≤35%). Sin embargo, este estudio tiene limitaciones significativas cuando se extrapola a la práctica de CTO: incluyó pacientes con EAC multivaso extensa y disfunción severa del VI (no CTOs aisladas), la población presentaba remodelado avanzado con potencial de recuperación inherentemente limitado, la técnica de ICP y completitud de la revascularización no fueron estandarizadas, y el estudio no tenía poder para detectar diferencias en subgrupos con FE preservada o CTO de vaso único. El REVIVED no anula el papel de la evaluación de viabilidad en CTO; refuerza que la selección de pacientes debe integrar estado de viabilidad, carga isquémica, severidad de síntomas y complejidad anatómica.
El estudio ISCHEMIA (NEJM, 2020) no mostró beneficio de mortalidad de la estrategia invasiva de rutina, pero demostró mejoría sintomática significativamente mayor con ICP, particularmente en pacientes con angina más severa.
ORBITA-CTO (JACC, 2026; Al-Lamee et al.): Este estudio sham-controlado aleatorizó 50 pacientes con CTO de vaso único, isquemia/viabilidad confirmadas, angina estable y J-CTO ≤3 a ICP de CTO vs. procedimiento placebo. A los 6 meses, el ICP de CTO mejoró significativamente el puntaje de síntomas de angina (OR 4,4; ICr 95% 1,6-12,7; Pr[Beneficio]=0,996), con ~31 días adicionales libres de angina vs. sham. Calidad de vida y clase CCS también mejoraron. Éxito técnico fue 96%, con ~30% requiriendo abordaje retrógrado. Sin muertes, IAM o retiros por empeoramiento de angina. Limitaciones: población altamente seleccionada (vaso único, J-CTO ≤3, operadores expertos), muestra pequeña (n=50). Aun así, ORBITA-CTO proporciona la primera evidencia placebo-controlada de que el ICP de CTO produce beneficio sintomático genuino más allá del efecto placebo en pacientes con isquemia y viabilidad documentadas.
Angiotomografía Coronaria para Planificación de CTO
La TCMD ha transformado la planificación pre-procedural de CTO proporcionando información anatómica 3D no disponible por angiografía convencional. Ventajas: cuantificación superior de calcificación, mejor definición del muñón proximal (especialmente en caps calcificados/ambiguos), medición precisa de longitud de oclusión, evaluación 3D del trayecto y tortuosidad del vaso.
Evaluación Morfológica por TC: Cuatro características críticas: (1) Muñón proximal: tapered favorece escalada anterógrada; blunt/ambiguo puede requerir técnicas subintimales o retrógrada; TC detecta micro-canales invisibles en angiografía. (2) Cuerpo de la oclusión: longitud, extensión de calcificación (arco de calcio, densidad en Hounsfield), micro-canales. (3) Tortuosidad: evaluación 3D exclusiva de TC. (4) Cap distal/vaso: calidad del vaso, tamaño de landing zone, anatomía de ramas para planificación de reentrada ADR.
Sistemas de Puntuación: J-CTO (Morino, 2011): cap abrupto, calcificación, tortuosidad >45°, longitud ≥20mm, intento previo; 0-5 puntos (0=Fácil 88%, ≥3=Muy Difícil 10%). CT-RECTOR (Opolski, 2015): puntuación específica de TC con mejor evaluación de calcificación y tortuosidad 3D. PROGRESS CTO (Christopoulos, 2016): tortuosidad proximal, ambigüedad del cap, localización CX, sin colaterales intervencionistas; VPP 87%. CASTLE (Alessandrino, 2019): incorpora factores del paciente (edad, CABG previo); 0-6 puntos, VPP 87%.
Técnicas Avanzadas de TC: TC con doble inyección (protocolo de contraste bifásico/secuencial) opacifica simultáneamente vasos proximal y distal. Reconstrucción 3D y planificación virtual (Synapse Vincent, Ziostation, Vitrea) permite trazado virtual, identificación de zona de reentrada y planificación retrógrada con visualización del trayecto septal. Fusión TC-angiografía proporciona roadmap en tiempo real durante fluoroscopia.
Cómo la TC Cambia la Estrategia Procedural
Selección de abordaje: cap blunt/ambiguo con calcificación severa → favorecer retrógrada o ADR. Selección de alambre: micro-canal en cap o morfología tapered → iniciar con alambre polymer-jacketed (Fielder XT-A, Gladius). Preparación de equipamiento: arco de calcio >270° → RotaPro/aterectomía orbital o IVL listos. Planificación de reentrada: landing zone 15mm proximal al takeoff de la PDA → objetivo para Stingray. Evaluación de colaterales: trayecto septal y tamaño de colateral epicárdica → seleccionar canal retrógrado. Evaluación de riesgo: CT-RECTOR ≥3 o J-CTO ≥3 con calcificación → planificar caso prolongado, discutir abordagem em etapas, asegurar disponibilidad de SCM.
Matriz de Decisión Práctica
Viable + Isquémico (LGE <50%, defecto al estrés): Indicación fuerte para ICP de CTO. Proceder con planificación por TC.
Viable + Sin Isquemia (LGE <50%, sin defecto): Considerar ICP de CTO para síntomas. Beneficio principalmente sintomático.
No viable + Isquémico (LGE >50%, defecto al estrés): Contraindicación relativa. Recuperación funcional limitada. ICP si angina refractaria o sustrato arrítmico.
No viable + Sin Isquemia (LGE >50%, defecto matched): ICP de CTO no recomendado. Cicatriz transmural, sin isquemia. Considerar evaluación de DAI.
Procedural Strategy: Access, Antegrade vs Retrograde
Vascular Access
Dual arterial access is the standard for CTO PCI. Contralateral injection is critical for real-time visualization of the distal vessel, collateral assessment, and wire position confirmation. Bilateral radial access (7Fr/6Fr or 7Fr/7Fr) is preferred for patient comfort and reduced vascular complications. Femoral access may be required for larger guide catheter support (8Fr) or when bilateral radial is not feasible. Triple access is occasionally needed for complex anatomy (e.g., dual injection plus additional support catheter, or combined antegrade/retrograde with separate collateral donor visualization).
The Hybrid Algorithm
The hybrid algorithm (Brilakis et al.) provides a systematic framework for CTO PCI strategy selection based on four angiographic characteristics: proximal cap ambiguity, occlusion length, distal vessel quality, and interventional collateral suitability. Primary antegrade wiring (AWE) is first-line for short occlusions (<20mm) with clear proximal cap and good distal target. Antegrade dissection re-entry (ADR) using CrossBoss/Stingray or LAST technique is preferred for longer lesions (>20mm) with clear proximal cap. Retrograde approach is selected when the proximal cap is ambiguous, the antegrade anatomy is unfavorable, or antegrade attempts have failed, provided suitable interventional collaterals exist (septal preferred over epicardial).
Retrograde Technique
The retrograde approach involves advancing a guidewire and microcatheter through collateral channels (septal or epicardial) to reach the distal true lumen of the CTO. Key techniques include: controlled retrograde tracking through collaterals using Sion, Suoh03, or Caravel-type wires; reverse CART (Controlled Antegrade and Retrograde subintimal Tracking) for connection between antegrade and retrograde subintimal spaces using balloon or knuckle wire dilation; and externalization using a long guidewire (RG3, R350) for subsequent balloon and stent delivery from the antegrade side. Collateral perforation remains the most feared complication and requires immediate management with fat embolization (epicardial) or covered stent/coil deployment.
Estratégia Procedural: Acesso, Anterógrada vs Retrógrada
Acesso Vascular
Duplo acesso arterial é o padrão para ICP de CTO. A injeção contralateral é crítica para visualização em tempo real do vaso distal, avaliação de colaterais e confirmação da posição do fio. Acesso birradial (7Fr/6Fr ou 7Fr/7Fr) é preferido pelo conforto do paciente e redução de complicações vasculares. Acesso femoral pode ser necessário para maior suporte do cateter-guia (8Fr) ou quando birradial não é viável. Triplo acesso é ocasionalmente necessário para anatomia complexa (ex: dupla injeção mais cateter de suporte adicional, ou anterógrada/retrógrada combinada com visualização separada do doador colateral).
Algoritmo Híbrido
O algoritmo híbrido (Brilakis et al.) fornece uma estrutura sistemática para seleção de estratégia baseado em quatro características angiográficas: ambiguidade do coto proximal, comprimento da oclusão, qualidade do vaso distal e adequação de colaterais intervencionistas. A escalada anterógrada de fio-guia (AWE) é primeira linha para oclusões curtas (<20mm) com coto proximal claro e bom alvo distal. A dissecção anterógrada e reentrada (ADR) com CrossBoss/Stingray ou técnica LAST é preferida para lesões mais longas (>20mm) com coto proximal claro. A abordagem retrógrada é indicada quando o coto proximal é ambíguo, a anatomia anterógrada é desfavorável ou tentativas anterógradas tenham falhado, desde que existam colaterais intervencionistas adequadas (septais preferidas em relação às epicárdicas).
Técnica Retrógrada
A abordagem retrógrada envolve avançar fio-guia e microcateter através de canais colaterais (septais ou epicárdicos) para alcançar o lúmen verdadeiro distal da CTO. Técnicas-chave incluem: navegação retrógrada controlada através de colaterais usando fios Sion, Suoh03 ou tipo Caravel; reverse CART (Controlled Antegrade and Retrograde subintimal Tracking) para conexão entre espaços subintimais anterógrado e retrógrado usando dilatação por balão ou knuckle wire; e externalização usando fio-guia longo (RG3, R350) para posterior entrega de balão e stent pelo lado anterógrado. Perfuração colateral é a complicação mais temida e requer manejo imediato com embolização de gordura (epicárdica) ou implante de stent coberto/coil.
Estrategia Procedural: Acceso, Anterógrada vs Retrógrada
Acceso Vascular
El doble acceso arterial es el estándar para ICP de CTO. La inyección contralateral es crítica para la visualización en tiempo real del vaso distal, evaluación de colaterales y confirmación de la posición del alambre. Acceso birradial (7Fr/6Fr o 7Fr/7Fr) es preferido por la comodidad del paciente y reducción de complicaciones vasculares. El acceso femoral puede ser necesario para mayor soporte del catéter guía (8Fr) o cuando el birradial no es factible. El triple acceso es ocasionalmente necesario para anatomía compleja (ej: doble inyección más catéter de soporte adicional, o anterógrada/retrógrada combinada con visualización separada del donante colateral).
Algoritmo Híbrido
El algoritmo híbrido (Brilakis et al.) proporciona un marco sistemático para la selección de estrategia basado en cuatro características angiográficas: ambigüedad del muñón proximal, longitud de la oclusión, calidad del vaso distal e idoneidad de colaterales intervencionistas. Escalada anterógrada de alambre (AWE) es primera línea para oclusiones cortas (<20mm) con muñón proximal claro y buen objetivo distal. Disección anterógrada y reentrada (ADR) usando CrossBoss/Stingray o técnica LAST es preferida para lesiones más largas (>20mm) con muñón proximal claro. El abordaje retrógrado se selecciona cuando el muñón proximal es ambiguo, la anatomía anterógrada es desfavorable o los intentos anterógrados han fallado, siempre que existan colaterales intervencionistas adecuadas (septales preferidas sobre epicárdicas).
Técnica Retrógrada
El abordaje retrógrado involucra avanzar alambre guía y microcatéter a través de canales colaterales (septales o epicárdicos) para alcanzar el lumen verdadero distal de la CTO. Las técnicas clave incluyen: navegação retrógrada controlada a través de colaterales usando alambres Sion, Suoh03 o tipo Caravel; reverse CART (Controlled Antegrade and Retrograde subintimal Tracking) para conexión entre espacios subintimales anterógrado y retrógrado usando dilatación con balón o knuckle wire; y externalización usando alambre guía largo (RG3, R350) para posterior entrega de balón y stent desde el lado anterógrado. La perforación colateral es la complicación más temida y requiere manejo inmediato con embolización de grasa (epicárdica) o despliegue de stent cubierto/coil.
Risks, Complications & Management
CTO PCI carries specific risks beyond standard PCI. Major adverse cardiac events (MACE) occur in 2-3% of cases in high-volume centers. Key complications and their management:
Coronary Perforation
Ellis classification guides management. Type I-II perforations (crater/pericardial staining without jet) are typically managed conservatively with prolonged balloon inflation and reversal of anticoagulation. Type III perforation (frank extravasation, ≥1mm jet) requires immediate covered stent deployment, pericardiocentesis if tamponade develops, and possible surgical consultation. Retrograde collateral perforation (septal: usually benign, self-limiting; epicardial: potentially catastrophic, requiring fat embolization or coil deployment).
Donor Vessel Compromise
Hemodynamic instability during CTO PCI can occur from prolonged occlusion of the donor vessel during contralateral injection. In patients with multivessel disease, consider mechanical circulatory support (Impella, ECMO) upfront for left main or last remaining vessel interventions.
Radiation and Contrast
CTO procedures typically require higher radiation doses (median air kerma 3-5 Gy) and contrast volumes (200-400mL). Strategies to minimize include: use of IVUS to reduce contrast (zero-contrast or ultra-low-contrast techniques), radiation-reduction protocols (low frame rate, collimation, table height optimization), and staged procedures when contrast limits are reached (typically 3.5x eGFR in mL).
Riscos, Complicações e Manejo
A ICP para CTO carrega riscos específicos além da ICP padrão. Eventos adversos cardíacos maiores (MACE) ocorrem em 2-3% dos casos em centros de alto volume. Principais complicações e seu manejo:
Perfuração Coronariana
A classificação de Ellis guia o manejo. Perfurações tipo I-II (cratera/impregnação pericárdica sem jato) são tipicamente manejadas conservadoramente com insuflação prolongada de balão e reversão da anticoagulação. Perfuração tipo III (extravasamento franco, jato ≥1mm) requer implante imediato de stent coberto, pericardiocentese se tamponamento se desenvolver e possível consulta cirúrgica. Perfuração colateral retrógrada (septal: geralmente benigna, autolimitada; epicárdica: potencialmente catastrófica, requerendo embolização de gordura ou implante de coil).
Comprometimento do Vaso Doador
Instabilidade hemodinâmica durante ICP de CTO pode ocorrer por oclusão prolongada do vaso doador durante injeção contralateral. Em pacientes com doença multiarterial, considere suporte circulatório mecânico (Impella, ECMO) de antemão para intervenções em tronco de coronária esquerda ou último vaso remanescente.
Radiação e Contraste
Procedimentos de CTO tipicamente requerem maiores doses de radiação (mediana de air kerma 3-5 Gy) e volumes de contraste (200-400mL). Estratégias para minimizar incluem: uso de IVUS para reduzir contraste (técnicas zero-contraste ou ultra-baixo contraste), protocolos de redução de radiação (baixo frame rate, colimação, otimização da altura da mesa) e procedimentos estagiados quando limites de contraste são atingidos (tipicamente 3.5x TFGe em mL).
Riesgos, Complicaciones y Manejo
El ICP para CTO conlleva riesgos específicos más allá del ICP estándar. Los eventos adversos cardíacos mayores (MACE) ocurren en 2-3% de los casos en centros de alto volumen. Principales complicaciones y su manejo:
Perforación Coronaria
La clasificación de Ellis guía el manejo. Las perforaciones tipo I-II (cráter/tinción pericárdica sin chorro) se manejan típicamente de forma conservadora con inflación prolongada de balón y reversión de la anticoagulación. La perforación tipo III (extravasación franca, chorro ≥1mm) requiere implante inmediato de stent cubierto, pericardiocentesis si se desarrolla taponamiento y posible consulta quirúrgica. Perforación colateral retrógrada (septal: generalmente benigna, autolimitada; epicárdica: potencialmente catastrófica, requiriendo embolización de grasa o despliegue de coil).
Compromiso del Vaso Donante
La inestabilidad hemodinámica durante ICP de CTO puede ocurrir por oclusión prolongada del vaso donante durante la inyección contralateral. En pacientes con enfermedad multivaso, considere soporte circulatorio mecánico (Impella, ECMO) de antemano para intervenciones en tronco de coronaria izquierda o último vaso remanente.
Radiación y Contraste
Los procedimientos de CTO típicamente requieren mayores dosis de radiación (mediana de air kerma 3-5 Gy) y volúmenes de contraste (200-400mL). Estrategias para minimizar incluyen: uso de IVUS para reducir contraste (técnicas cero-contraste o ultra-bajo contraste), protocolos de reducción de radiación (baja tasa de cuadros, colimación, optimización de altura de mesa) y procedimientos escalonados cuando se alcanzan límites de contraste (típicamente 3.5x TFGe en mL).
Complex and High-Risk PCI
Left Main PCI
The EXCEL and NOBLE trials established non-inferiority of ICP versus CABG for left main disease in appropriate candidates. Left main PCI requires meticulous lesion assessment, staged procedures when necessary, and consideration of hemodynamic support for high-risk anatomy. Provisional single-stent strategy is preferred when feasible.
Bifurcation Management
Contemporary bifurcation strategies emphasize provisional stenting with main branch optimization. Two-stent techniques (culotte, crush, DK-crush) reserved for cases with large, diseased side branches. The IVUS-guided provisional approach reduces restenosis compared to routine two-stent strategies.
Calcified Lesion Treatment
Severely calcified lesions present unique challenges. Techniques include: Intravascular Lithotripsy (IVL) for sonic pulse energy disruption of calcium; Rotational Atherectomy for elliptical debulking; Orbital Atherectomy with flexible shaft technology; and Laser Angioplasty for fibrocalcific plaque.
Hemodynamic Support
High-risk PCI increasingly incorporates mechanical circulatory support. Impella devices provide up to 5.0L/min support with active unloading. ECMO offers higher flow for cardiogenic shock scenarios. Careful patient selection, timing, and post-procedure weaning protocols optimize outcomes.
Rotational Atherectomy with IVUS-Guided Optimization
ICP Complexa e de Alto Risco
ICP de Tronco de Coronária Esquerda
Os ensaios EXCEL e NOBLE estabeleceram não-inferioridade de ICP versus CABG para doença de tronco de coronária esquerda em candidatos selecionados. ICP de tronco principal requer avaliação meticulosa de lesão, procedimentos em estágios quando necessário, e consideração de suporte hemodinâmico para anatomia de alto risco. A estratégia de stent provisório é preferida quando factível.
Manejo de Bifurcação
As estratégias contemporâneas de bifurcação priorizam o stenting provisório com otimização do ramo principal. Técnicas de dois stents (culotte, crush, DK-crush) são reservadas para ramos laterais significativos comprometidos. A estratégia provisória guiada por IVUS reduz a reestenose em comparação com a abordagem rotineira de dois stents.
Tratamento de Lesões Calcificadas
Lesões severamente calcificadas requerem técnicas especializadas: Litotripsia Intravascular (IVL) para fratura do cálcio por ondas de choque; Aterectomia Rotacional (RotaPro) para desbastamento elíptico; Aterectomia Orbital (CSI) com tecnologia de haste flexível; e Laser Excimer para placa fibrocálcica.
Suporte Hemodinâmico
ICP de alto risco cada vez mais incorpora suporte circulatório mecânico. Dispositivos Impella fornecem suporte de até 5,0 L/min com descarregamento ativo do VE. ECMO oferece suporte hemodinâmico completo em cenários de choque cardiogênico. Seleção criteriosa de pacientes, timing adequado e protocolos de desmame pós-procedimento otimizam os resultados.
Aterectomia Rotacional com Otimização Guiada por IVUS
ICP Complejo y de Alto Riesgo
ICP de Tronco Principal Izquierdo
Los ensayos EXCEL y NOBEL establecieron la no-inferioridad del ICP versus CABG para la enfermedad del tronco principal en candidatos apropiados. El ICP del tronco principal requiere una evaluación meticulosa de las lesiones, procedimientos escalonados cuando sea necesario, y consideración del soporte hemodinámico para la anatomía de alto riesgo. La estrategia de stent único provisional es preferida cuando es posible.
Gestión de Bifurcación
Las estrategias contemporáneas de bifurcación enfatizan el stenting provisional con optimización de la rama principal. Las técnicas de dos stents (culotte, crush, DK-crush) se reservan para casos con grandes ramas laterales enfermas. El enfoque provisional guiado por IVUS reduce la reestenosis comparado con estrategias rutinarias de dos stents.
Tratamiento de Lesiones Calcificadas
Las lesiones severamente calcificadas presentan desafíos únicos. Las técnicas incluyen: Litotricia Intravascular (IVL) para interrupción de calcio por energía de pulso sónico; Aterectomía Rotacional para desbridamiento elíptico; Aterectomía Orbital con tecnología de eje flexible; y Angioplastia con Láser para placa fibrocalcífica.
Soporte Hemodinámico
El ICP de alto riesgo cada vez más incorpora soporte circulatorio mecánico. Los dispositivos Impella proporcionan soporte de hasta 5.0L/min con descarga activa. ECMO ofrece tasas de flujo más altas para escenarios de choque cardiogénico. La selección cuidadosa de pacientes, el momento y los protocolos de destete post-procedimiento optimizan los resultados.
Aterectomía Rotacional con Optimización Guiada por IVUS
Intravascular Imaging Guidance
IVUS vs. OCT: Clinical Applications
IVUS: Superior for assessment of vessel size and plaque burden. Penetration depth (~4-5mm) allows interrogation of vessel walls. Excellent for calcification evaluation and chronic occlusion assessment.
OCT: Resolution (~10-15 microns vs. 150 for IVUS) enables detection of thin-cap fibroatheromas and subtle stent malapposition. Superior for edge dissection and tissue prolapse assessment. Limited penetration (~2mm) in calcified vessels.
Optimization Endpoints
IVUS-guided optimization targets minimal stent area (MSA) >80% of distal reference vessel, complete lesion coverage, and expansion ratio >80%. OCT optimization focuses on mean stent area (typically >5.5mm² for left main), coverage of all side branches, and absence of edge dissection >200 microns or malapposition >200 microns.
IVUS + OCT (Co-registration 1)
IVUS + OCT (Co-registration 2)
Orientação de Imagem Intravascular
IVUS vs. OCT: Aplicações Clínicas
IVUS: Superior para avaliação do diâmetro do vaso e carga de placa. Profundidade de penetração (~4-5 mm) permite avaliação completa da parede vascular. Excelente para avaliação de calcificação e de oclusões crônicas.
OCT: Resolução (~10-15 micrômetros vs. 150 para IVUS) permite detecção de fibroateromas de capa fina (TCFA) e má aposição sutil de stent. Superior para avaliação de dissecção de borda e prolapso de tecido. Penetração limitada (~2mm) em vasos calcificados.
Pontos de Otimização
A otimização guiada por IVUS visa área mínima de stent (MSA) >80% do vaso de referência distal, cobertura completa de lesão e razão de expansão >80%. A otimização OCT se concentra na área média de stent (tipicamente >5,5mm² para tronco principal), cobertura de todos os ramos laterais e ausência de dissecção de borda >200 micrômetros ou má aposição >200 micrômetros.
IVUS + OCT (Co-registro 1)
IVUS + OCT (Co-registro 2)
Guía de Imágenes Intravasculares
IVUS vs. OCT: Aplicaciones Clínicas
IVUS: Superior para la evaluación del tamaño del vaso y la carga de placa. La profundidad de penetración (~4-5mm) permite la interrogación de las paredes de los vasos. Excelente para la evaluación de la calcificación y la evaluación de la oclusión crónica.
OCT: La resolución (~10-15 micrómetros vs. 150 para IVUS) permite la detección de fibroateromas de capa delgada y mala aposición sutil del stent. Superior para la evaluación de la disección de borde y el prolapso de tejido. La penetración limitada (~2mm) en vasos calcificados.
Puntos Finales de Optimización
La optimización guiada por IVUS tiene como objetivo un área mínima de stent (MSA) >80% del vaso de referencia distal, cobertura completa de lesiones y razón de expansión >80%. La optimización de OCT se enfoca en el área media de stent (típicamente >5,5mm² para tronco principal), cobertura de todas las ramas laterales y ausencia de disección de borde >200 micrómetros o mala aposición >200 micrómetros.
IVUS + OCT (Co-registro 1)
IVUS + OCT (Co-registro 2)
Post-Procedure Management & Follow-Up
Post-CTO PCI management follows standard PCI guidelines with specific considerations for the complexity of the procedure.
Antiplatelet Therapy
DAPT duration follows ARC-HBR criteria and current guidelines. Standard recommendation is 12 months of DAPT (aspirin + P2Y12 inhibitor). In patients at high bleeding risk, shorter DAPT (1-3 months) followed by P2Y12 monotherapy is acceptable per TWILIGHT and STOPDAPT-2 data. Extended DAPT beyond 12 months may be considered for patients with high ischemic risk and low bleeding risk.
Surveillance
Clinical follow-up at 1 month, 3 months, and annually thereafter. Functional testing at 6-12 months is recommended, particularly if symptoms recur. Routine angiographic surveillance is not recommended unless clinically indicated. IVUS-optimized stent deployment at the index procedure reduces the need for target vessel revascularization and should be standard practice.
Risk Factor Modification
Aggressive secondary prevention: LDL target <55 mg/dL (ESC) or <70 mg/dL (ACC/AHA), HbA1c <7%, blood pressure <130/80, smoking cessation, and cardiac rehabilitation referral. These measures are critical for long-term stent patency and event-free survival.
Manejo Pós-Procedimento e Seguimento
O manejo pós-ICP de CTO segue as diretrizes padrão de ICP com considerações específicas para a complexidade do procedimento.
Terapia Antiplaquetária
A duração da DAPT segue os critérios ARC-HBR e as diretrizes vigentes. A recomendação padrão é 12 meses de DAPT (aspirina + inibidor P2Y12). Em pacientes com alto risco de sangramento, DAPT mais curta (1-3 meses) seguida de monoterapia com P2Y12 é aceitável conforme dados do TWILIGHT e STOPDAPT-2. DAPT estendida além de 12 meses pode ser considerada para pacientes com alto risco isquêmico e baixo risco hemorrágico.
Vigilância
Seguimento clínico em 1 mês, 3 meses e anualmente a partir de então. Prova funcional entre 6 e 12 meses é recomendada, particularmente se sintomas recorrerem. Vigilância angiográfica de rotina não é recomendada a menos que clinicamente indicada. A otimização do implante de stent guiada por IVUS no procedimento índice reduz a necessidade de revascularização do vaso-alvo e deve ser prática rotineira.
Modificação de Fatores de Risco
Prevenção secundária agressiva: alvo de LDL <55 mg/dL (ESC) ou <70 mg/dL (ACC/AHA), HbA1c <7%, pressão arterial <130/80, cessação do tabagismo e encaminhamento para reabilitação cardíaca. Estas medidas são críticas para patência do stent a longo prazo e sobrevida livre de eventos.
Manejo Post-Procedimiento y Seguimiento
El manejo post-ICP de CTO sigue las guías estándar de ICP con consideraciones específicas para la complejidad del procedimiento.
Terapia Antiplaquetaria
La duración de DAPT sigue criterios ARC-HBR y guías actuales. La recomendación estándar es 12 meses de DAPT (aspirina + inhibidor P2Y12). En pacientes con alto riesgo de sangrado, DAPT más corta (1-3 meses) seguida de monoterapia con P2Y12 es aceptable según datos de TWILIGHT y STOPDAPT-2. DAPT extendida más allá de 12 meses puede considerarse para pacientes con alto riesgo isquémico y bajo riesgo hemorrágico.
Vigilancia
Seguimiento clínico al mes, 3 meses y anualmente después. Prueba funcional a los 6-12 meses es recomendada, particularmente si los síntomas recurren. La vigilancia angiográfica de rutina no es recomendada a menos que esté clínicamente indicada. El implante de stent optimizado por IVUS en el procedimiento índice reduce la necesidad de revascularización del vaso objetivo y debe ser práctica estándar.
Modificación de Factores de Riesgo
Prevención secundaria agresiva: objetivo de LDL <55 mg/dL (ESC) o <70 mg/dL (ACC/AHA), HbA1c <7%, presión arterial <130/80, cesación del tabaquismo y derivación a rehabilitación cardíaca. Estas medidas son críticas para la permeabilidad del stent a largo plazo y la supervivencia libre de eventos.
Referring a Patient
We welcome referrals for patients with chronic total occlusions, complex multivessel disease, left main interventions, heavily calcified lesions, and refractory angina unsuitable for medical management alone.
What to Send
Most recent coronary angiography (digital or physical, preferably multiple projections)
Clinical summary including presentation, medications, and comorbidities
Prior intervention history and any imaging (IVUS, OCT, angiography)
Current functional status and symptom burden
Left ventricular ejection fraction and echocardiography when available
Contact Information
Referrals can be submitted through our main website contact page or directly through electronic health systems if integrated. For urgent consultations or complex cases, please call directly. We typically schedule consultations within 1-2 weeks. A multidisciplinary heart team discussion is encouraged for complex anatomy.
Encaminhando um Paciente
Recebemos encaminhamentos de pacientes com oclusões totais crônicas, doença multivaso complexa, intervenções de tronco principal, lesões fortemente calcificadas e angina refratária a terapia médica otimizada.
O que Enviar
Angiografia coronariana mais recente (digital ou física, de preferência múltiplas projeções)
Resumo clínico incluindo quadro clínico, medicações em uso e comorbidades
Histórico de intervenções prévias e exames de imagem (IVUS, OCT, angiografia)
Classe funcional atual e carga sintomática
Fração de ejeção do VE e ecocardiograma recente, quando disponíveis
Informações de Contato
Os encaminhamentos podem ser realizados pela página de contato do nosso site principal ou diretamente por sistemas eletrônicos de saúde integrados. Para consultas urgentes ou casos complexos, entre em contato diretamente. O agendamento é realizado em 1 a 2 semanas. Discussão em Heart Team é encorajada para anatomia complexa.
Derivar un Paciente
Bienvenidas las derivaciones para pacientes con oclusiones totales crónicas, enfermedad multivaso compleja, intervenciones del tronco principal, lesiones fuertemente calcificadas y angina refractaria inadecuada para manejo médico solo.
Qué Enviar
Angiografía coronaria más reciente (digital o física, preferiblemente múltiples proyecciones)
Resumen clínico incluyendo presentación, medicamentos y comorbilidades
Historial de intervención anterior e cualquier imagen (IVUS, OCT, angiografía)
Estado funcional actual y carga de síntomas
Fracción de eyección ventricular izquierda y ecocardiografía cuando esté disponible
Información de Contacto
Las derivaciones se pueden enviar a través de la página de contacto de nuestro sitio web principal o directamente a través de sistemas electrónicos de salud si está integrado. Para consultas urgentes o casos complejos, llame directamente a la oficina. Generalmente programamos consultas dentro de 1-2 semanas. Se recomienda una discusión multidisciplinaria del equipo cardíaco para anatomía compleja.
Ready to Discuss a Complex Case?
Referrals for CTO PCI, complex coronary intervention, and advanced imaging are welcome.
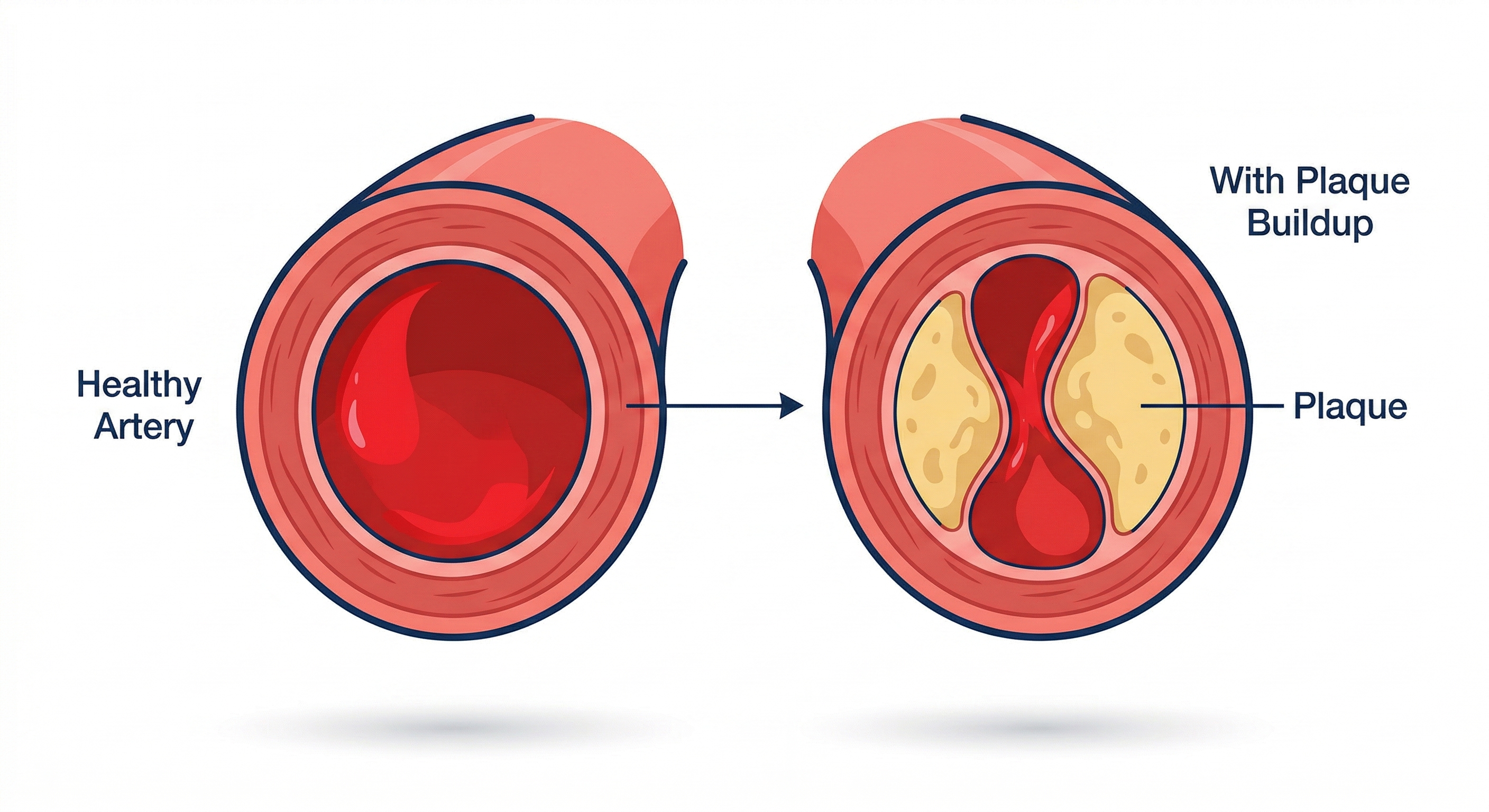 Healthy Artery vs. Plaque Buildup
Healthy Artery vs. Plaque Buildup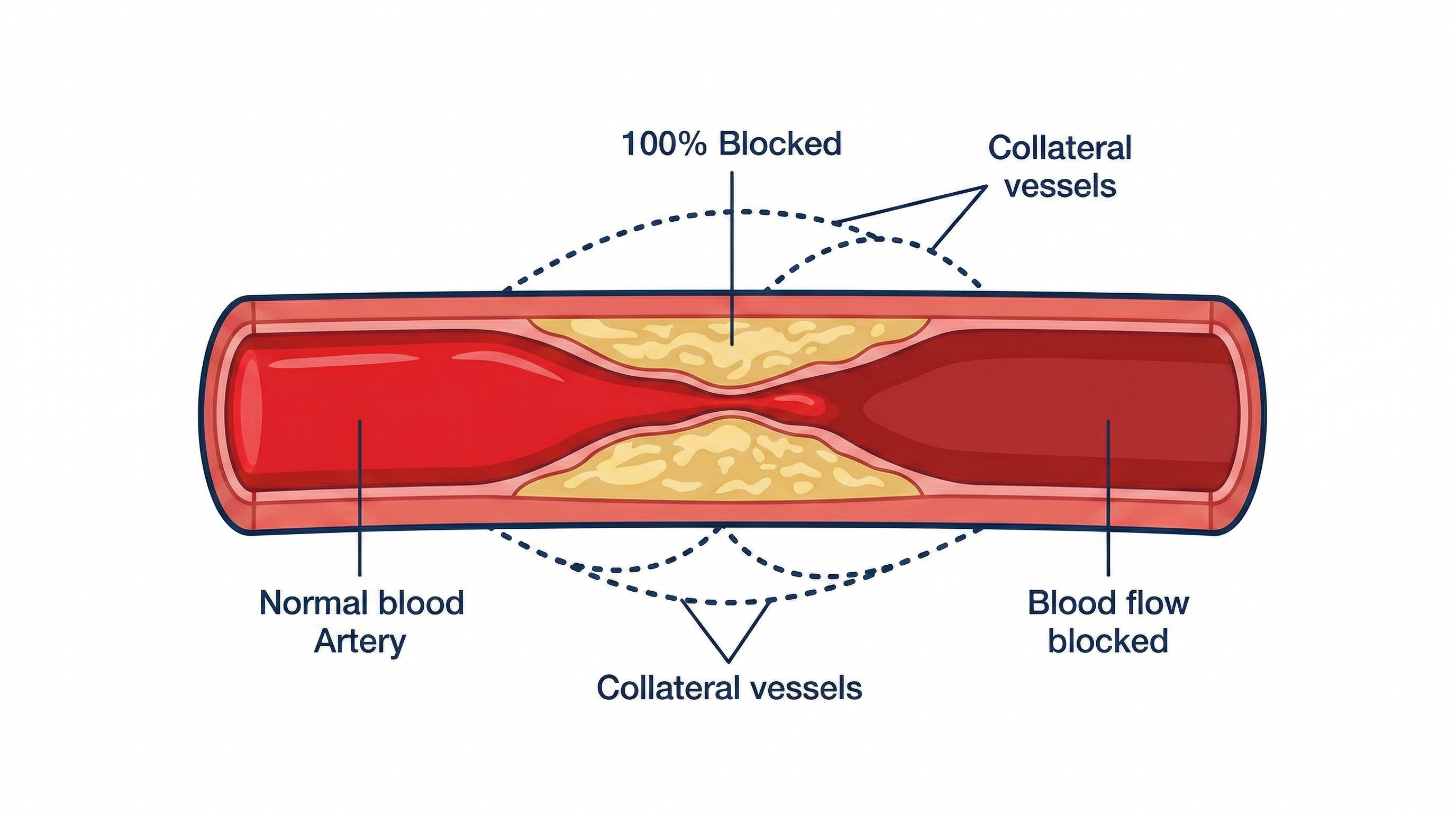 Chronic Total Occlusion (100% Blocked)
Chronic Total Occlusion (100% Blocked)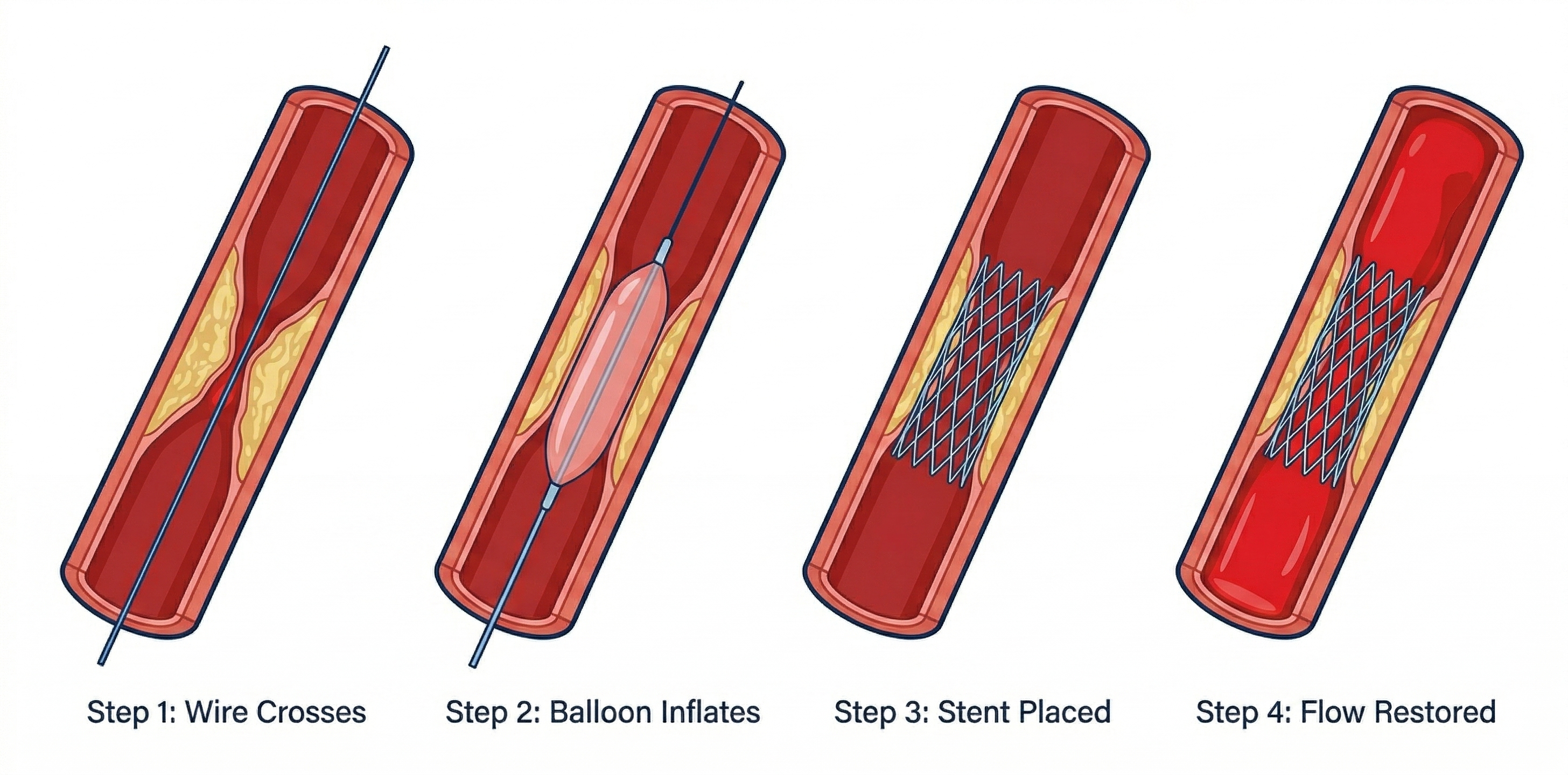
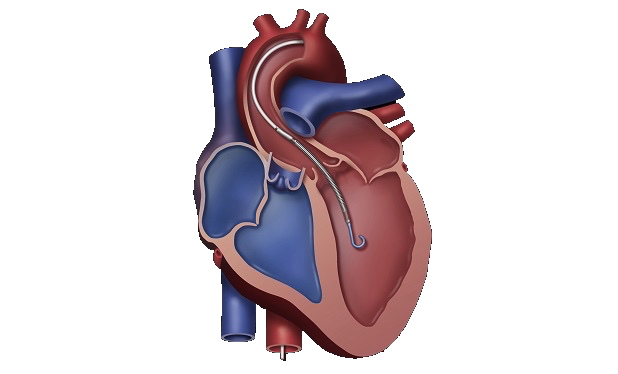 Coronary Intervention with Mechanical Circulatory Support (Impella)
Coronary Intervention with Mechanical Circulatory Support (Impella) Before: Complete Occlusion
Before: Complete Occlusion After: Flow Restored
After: Flow Restored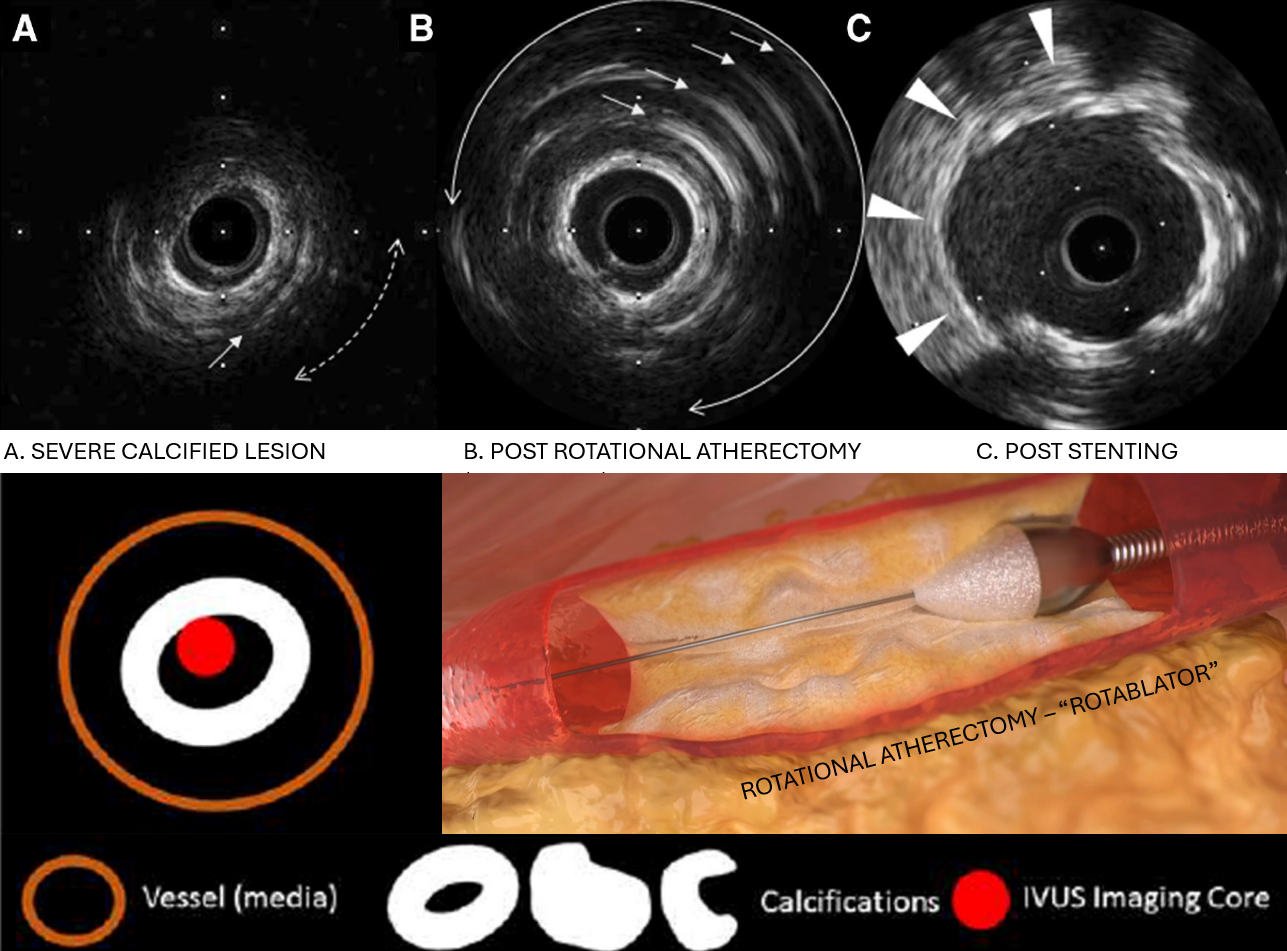 Rotational Atherectomy with IVUS-Guided Optimization
Rotational Atherectomy with IVUS-Guided Optimization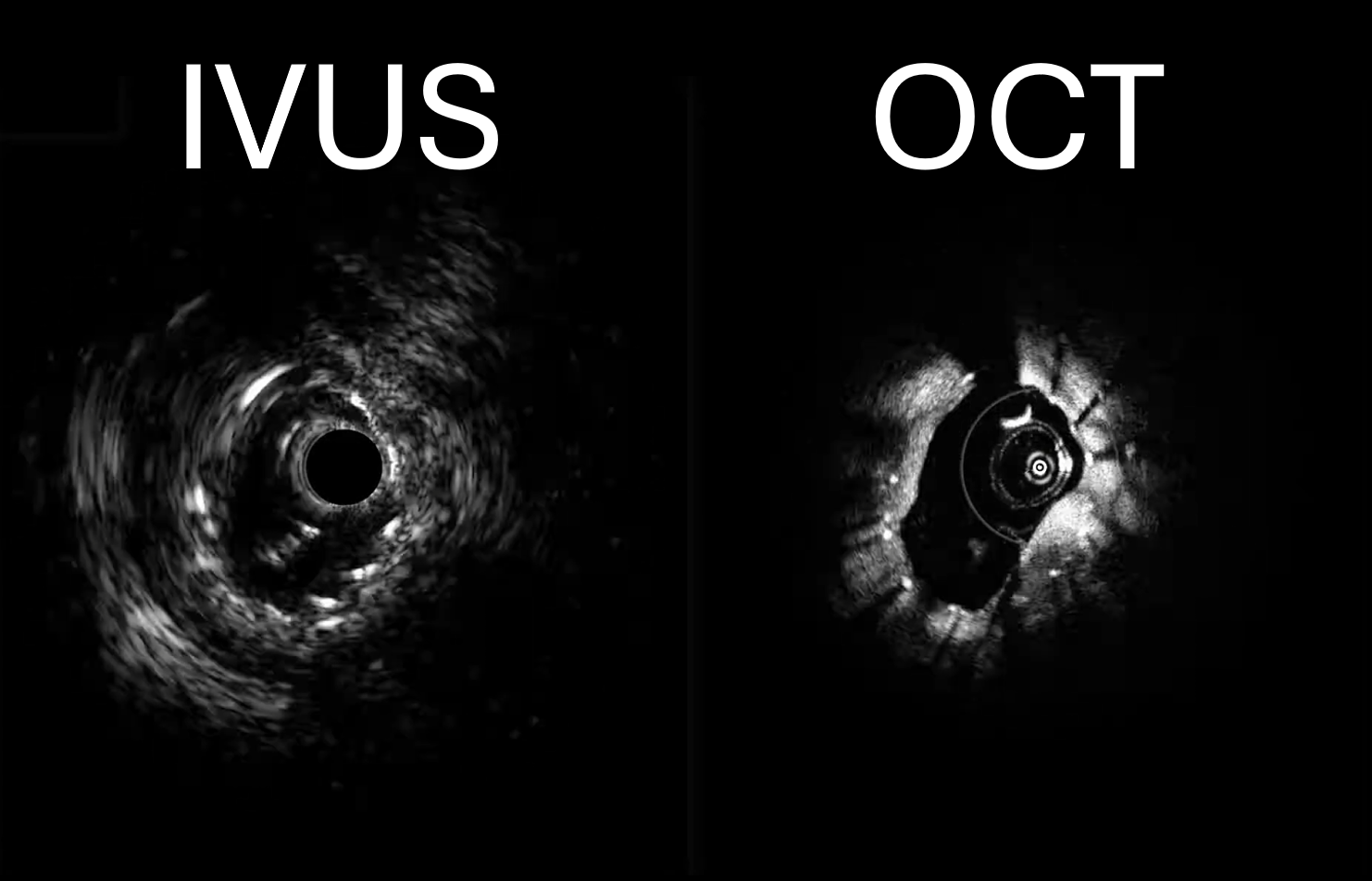 IVUS + OCT (Co-registration 1)
IVUS + OCT (Co-registration 1)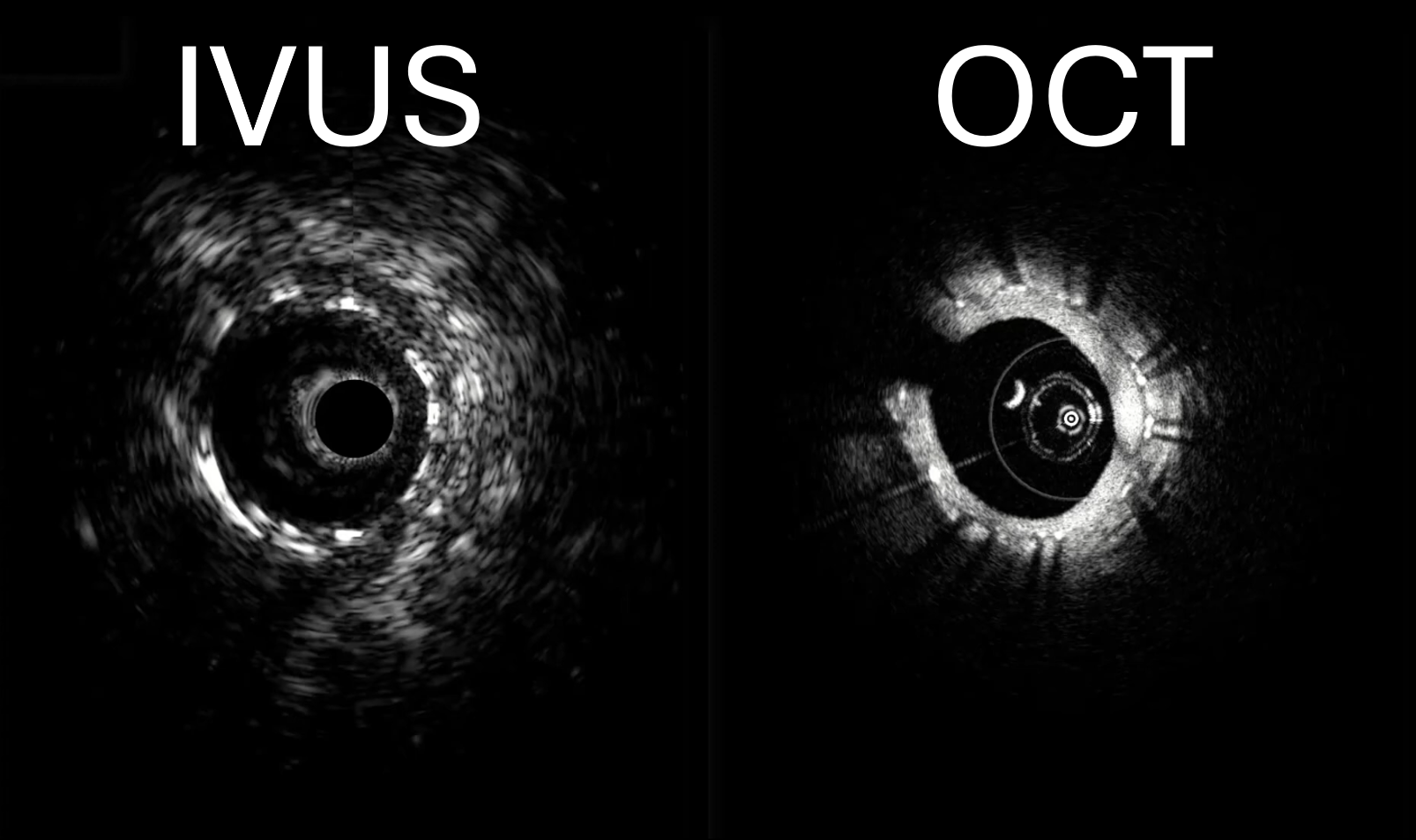 IVUS + OCT (Co-registration 2)
IVUS + OCT (Co-registration 2)